Author: admin
Summary
New Zealand is facing a serious threat to the nation’s health from COVID-19. Thus far, the health system has coped well. We currently have over 1300 cases with little evidence of strain or excess premature death.
The government and its advisors have articulated a strategy of ongoing lockdowns of New Zealand society for the foreseeable future in an attempt to eradicate the virus. We believe that holding out for vaccine development or pursuing an aggressive eradication policy are not realistic.
We are a group of academics who are concerned that such a strategy is not proportional to the threat posed by COVID-19 to New Zealanders’ health and that it is likely to substantially harm the nation’s long-term health and well-being, social fabric, economy, and education.
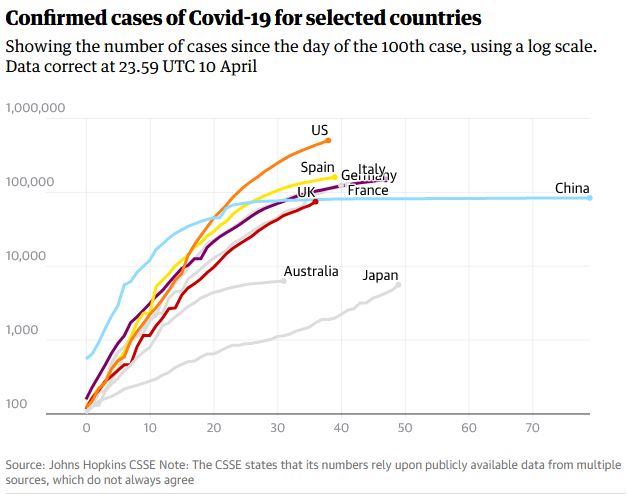
We recognise that COVID-19 has overwhelmed some hospitals overseas, with overflowing intensive care units in some densely populated cities, such as New York, and Milan. This is the principal risk posed by the transmission of the virus and we seek to avoid such a situation in New Zealand. In some European countries, there is excess mortality attributable to these outbreaks. Rest homes are especially vulnerable to outbreaks caused by the virus.
We believe that such a scenario is less likely to occur in New Zealand due to our lower population density. We also see that Australia, a country with greater population density in some regions, but in many respects, similar to ours, has seen sharply reducing disease incidence for several weeks, despite having a more relaxed lockdown policy.
We believe that it is in the best interests of the country to rapidly transition to a situation similar to the government’s alert level 2, while closely monitoring the spread of the virus and its impact on the health system. This would enable the majority of businesses to continue to operate and schools and universities to open. It would also allow essential domestic travel to resume.
We believe that an exclusive focus on the number of new cases of COVID-19 is less important than measures of whether or not the spread of the virus is causing an increase from background rates of hospital admissions, premature deaths, and intensive care bed occupancy. These latter measures are more important than the former in terms of deciding whether or not the country should be placed under strict lockdown in the future.
A focus of our response to the virus must incorporate returning to normality as soon as possible.The likely course of the virus is that many individuals will be infected with the virus and immunity in the population will develop. We understand that laboratory services are currently stretched by focus on PCR tests for the virus. However, we believe serosurveys of immunity would provide valuable information about the extent that the community has been exposed to the virus.
Up until now, the government has been selective in the information it is choosing to share with New Zealanders. We do not have a clear picture of what the government’s response will be in the next nine months and have had to guess this from comments of its advisors. We have not been told that spare capacity at Auckland hospitals is currently high, for example. We believe that New Zealanders should be free to debate the direction that the country will take in the next nine months, and that transparency should be a guiding principle for leading the country through this crisis.
What is COVID-19 and SARS-CoV-2?
SARS-CoV-2 belongs to a large group of viruses called “coronaviruses” that cause diseases in animals and humans. The first case of pneumonia associated with the virus was reported from Wuhan city, China, on the 12th of December 2019, and the outbreak was reported to the World Health Organisation on the 31st of December 2019. Cases had a shared history of exposure to Huanan seafood markets, indicating a likely animal source.
Six types of coronaviruses are known to affect humans. Four cause common cold type symptoms and two others cause severe illness: middle east respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS). The clinical syndrome associated with this virus is called COVID-19, and is characterised by cough, muscle aches and shortness of breath. Hospitalised patients develop pneumonia or lung infection. The diagnosis is made by a genetic test for the virus (PCR) from a swab taken from the back of the nose. Some patients who develop the pneumonia require mechanical ventilation in intensive care units. Conversely, about 50% of people who test positive for the virus have no symptoms in community surveys of the disease carried out in Iceland.
Now, more than 1.2 million test positive cases have occurred worldwide. The first case occurred in New Zealand on the 28th February 2020. At the time of writing (Sunday 12th April 2020), New Zealand had a total of 1,330 cases, with 14 currently in hospital, five in intensive care and four deaths. Deaths so far have occurred in people aged in their seventies to nineties with comorbidities. We do not have sufficient details to assess, but it is likely that some of these deaths were with the virus rather than a direct result of infection.
The rapid spread of COVID-19 has posed a risk to the health of populations. For example, intensive care units in several countries (for example: Italy, Spain and New York) were overwhelmed with a sharp rise in the number of cases which require mechanical ventilation, such that hospital facilities and personnel are substantially stretched. This increases the risk of transmission of the virus to other elderly patients and to staff.
What has New Zealand done to contain the virus in the short term?
New Zealand has introduced wide ranging and tough border restrictions on international visitors. Large gatherings were progressively banned. On March 25th New Zealand went into “lockdown”, including the closure of schools and non-essential businesses. Since the lockdown, new case numbers per day have stabilised and recently started to decline.
What is the government’s long-term plan?
The government has not clearly articulated a long term plan to address the threat. Government advisors have articulated such strategies such as waiting for the development of a vaccine and elimination of the virus, which would entail prolonged lockdowns.
Why are we challenging the New Zealand Government’s response?
The risks of the virus have been overstated
It is clear now that much of the modelling related to the mortality associated with COVID-19 was overestimated, including for New Zealand. In early March, the World Health Organization reported a Case Fatality Rate (the proportion of deaths that occur in individuals who are test-positive for SARS-CoV-2) of 3.4%, but this crude measure ignores undetected infections in people with no symptoms and therefore likely overstates the true CFR. New Zealand’s own modelling in late March predicted that 80,000 kiwis would die without mitigation measures (a CFR 1.6%) and based on the assumption that all New Zealanders would be infected – a highly unlikely scenario.
But now, with time, the picture is becoming clearer. With over 1300 confirmed and probable cases and four deaths, the overall CFR in New Zealand is approximately 0.30%. No deaths have yet occurred in people under the age of seventy. This overall CFR rate is similar to that seen for seasonal flu epidemics and indicates that the virus poses a low risk of fatality to the vast majority of people. As Dr Jay Bhattachayra (Professor of Medicine at Stanford University, USA) points out – the response, and the policies and strategies to stop the spread of an epidemic virus strain must be commensurate with the threat posed by the disease.
Since the average age of COVID-19 deaths has been in people aged 80 years, a large majority of cases have occurred from their comorbidities rather than from the virus alone – as is the case with all New Zealand’s deaths to date. An analysis by Professor David Spiegelhalter at Cambridge University shows that the CFR from the disease is conservatively estimated to be about the same as an individual’s average annual fatality rate. In effect, it is like squeezing a year’s mortality risk into two weeks. In Italy, a review found that just 12% of reported COVID-19 deaths were likely to be directly due to the disease. As Stanford epidemiologist Professor John Ioannides remarks of COVID-19: “it is only this year that every single case and every single death gets red alert broadcasting in the news.” In the past, such deaths would have not been attributed to a single virus, since extensive testing for these viruses had not been carried out.
The majority of severe outbreaks of COVID-19 globally have occurred in regions with very high population density, including London, Milan, New York, Wuhan and Madrid. Auckland, in contrast, has at least one third lower population density than the least populated of these cities. Population density is likely to be an important factor in the transmission of the virus, resulting in overwhelming limited health facilities.
Eradication of the virus while desirable is highly unrealistic
While laudable, the focus of the government has been on eradication of the virus. We believe this to be unrealistic. To date, no country has successfully eradicated a virus like COVID-19 that causes a high proportion of asymptomatic infection. The usual course during an epidemic is for susceptible individuals to get infected and develop immunity so that eventually the virus has nowhere to go. We agree with the widespread approach of ‘flattening the curve’ which seeks to reduce rapid spread so that cases can be accommodated by the health system.
The diagnostic test (PCR) used to identify cases is not sensitive. This is demonstrated by the growing number of test-negative positive cases with compatible symptoms who have had contact with positive cases. This means that the test is not ideal, and it will, therefore, be almost impossible to tell for certain whether the virus has been eradicated.
Complicating the eradication strategy is that the virus is likely to be more widely dispersed in the community than has been appreciated. For example, community studies from Iceland show that the population has high levels of asymptomatic test-positive cases. Half of the test-positive cases are asymptomatic. Such a study has not been done in New Zealand. Instead, allowing the population to develop immunity, which is a natural defense for the virus after infection could occur, and manage the spread of the virus while protecting those most vulnerable from the disease.
A German study in the town of Gangelt showed that about 2% of the population tested positive by PCR, indicating current viral infection. One in seven subjects (14%) had evidence of immunity to the virus, indicating that they will have low risk of re-infection. This means that in many countries, the virus has spread much further than is indicated by tracking new cases of PCR test-positive people. Until such a study is carried out in New Zealand, we can not determine this.
New Zealand cannot “hunker-in-a-bunker” until there’s a vaccine for a virus that is likely to become endemic in the rest of the world. Tourism, for example, is one of our most important industries, with annual tourism expenditure in New Zealand of $40.9 billion – that’s $112 million per day. Under an elimination scenario – we would lose our entire tourism sector as it is highly unlikely any tourists would incorporate a 2-week quarantine period into the start of their NZ holiday schedule. We cannot shut ourselves off from the world as we attempt to eliminate the virus and await the hopeful arrival of a vaccine that may take several years.
Managing risk to the health system
One of the risks of COVID-19 to a nation is the potential to overwhelm a healthcare system, particularly with respect to capacity to treat patients who require mechanical ventilation. New Zealand currently has 153 dedicated intensive care beds. However, in a crisis, the Ministry has indicated that up to 520 ventilators are available. In New Zealand only a small percentage of cases have required hospital treatment and even fewer require intensive care after a thousand test-positive cases. Hospitals are now at ~50% of their total capacity. Clearly, up to now, the virus has not had the devastating effect on hospital services as it was thought to. A managed spread would lower the rate of spread to levels that do not overwhelm health services.
A prolonged lockdown – the social and economic effects
This is the first ‘lockdown’ in New Zealand’s history. Small businesses are particularly vulnerable, especially those reliant on overseas visitors. We are already seeing a spike in unemployment claims and business insolvencies. The human cost of job losses and bankruptcies will be massive. In Spain, after a prolonged lockdown, unemployment percentages are now doubling every week while in the USA new jobless claims have exceeded 16 million. The impact on the global economy will likely be as heavy as the great depression.
Civil liberties in New Zealand are now eroded with unchecked State of Emergency powers. Confidence in the police is undermined. With the single focus of the health sector on COVID-19, important other treatment is being forgone, such as cancer surgery.
A prolonged lock-down and subsequent economic decline will also have numerous other implications like increased poverty, mental health problems and deaths. During the lockdown families will be unable to celebrate births and support their new family. Husbands, wives, sons daughters and other fr will be unable to comfort or say goodbye to some of the approximately 2,700 people who will have died in New Zealand due to natural causes over the four week lock-down period. This was detailed by Dr Elana Curtis (Te Arawa) from a Māori perspective. It will even impact our Predator Free 2050 ambitions and harm our native Taonga like kiwi. The evidence for the most aggressive lock-down measures is lacking and much of the pain of this shut-down will be borne by the socio-economically disadvantaged and our younger members of society.
Lastly, there is a real risk of damaging our ability to manage future pandemics – “over-reaction may damage the reputation of science, public health, media, and policy makers. It may foster disbelief that will jeopardize the prospects of an appropriately strong response if and when a more major pandemic strikes in the future.”
What should New Zealand do in the next nine months?
Cases are now in decline. We understand the decision to lockdown given the lack of data. But, it is now clear that COVID-19 affects different people and populations differently. We believe that the risk posed by the virus to the vast majority of the population does not justify ongoing lockdowns, which entail serious social, educational and economic consequences. We should, therefore, plan for coming out of lockdown by defining and stratifying risk groups.
New Zealand has enacted an efficient system for case identification and quarantine to contain the risk of further spread after imported cases were initially detected from overseas. Hospitals have also gone to great lengths to prepare for new cases.
Where our opinion differs from current policy is that we should now prepare to come out of lockdown and move to a situation similar to alert level 2 at the end of the four week lockdown period. Evidence from Australia indicates this is safe to do. Despite far less stringent lockdown rules, their new infection rates have been sharply declining for the last three weeks. This is also in Australian cities which have a higher population density than Auckland, such as Melbourne and Sydney. This would allow most businesses to open, and allow schools and Universities to reopen. Domestic travel should also be opened. South Korea and Singapore have followed such a strategy.
At a community level, we seek to avoid a situation in which clinical and public health response to the virus is overwhelmed. We believe that hospitals should be monitored for overcrowding and limited capacity in intensive care. At the time of writing, Auckland hospitals are at half capacity and not overwhelmed. This is the principal factor which should guide intensification of social distancing measures. Similarly, adequate capacity should be afforded to include adequate contact tracing and quarantine of newly identified cases.
We believe that testing of populations for serological evidence of immunity would help us better understand the threat posed by the virus. We understand that laboratory resources are currently stretched. However, such a study would give crucial information about exposure to the virus that would be useful for guiding further policy to contain the risks posed. This would be especially important for people who are at raised risk of fatality from the virus.
We agree that mass gatherings (>100 people) should be cancelled. Isolation of rest homes is especially important. People who are at high risk of severe complications of the disease, by virtue of age and sickness remain at home, with state funded support provided to maintain such people in good health. Given the high rate of imported cases, we agree that entry border measures remain maximised.
We believe that an exclusive focus on the number of new cases of COVID-19 is less important than measures of whether or not the spread of the virus is causing an increase from background rates of hospital admissions, premature deaths, and intensive care bed occupancy. These latter measures are more important than the former in terms of deciding whether or not the country should be placed under strict lockdown in the future.
We believe the government should be open about how it is making far reaching decisions about New Zealand’s future. We have seen some information shared, however, much is kept secret. We have not been clearly told what the government’s future strategy to address the pandemic is. With such high stakes, we believe the government needs to be transparent about sharing its decision making with its constituents.
Our 10 point plan
- Low risk people should be allowed to return to their normal daily activities. For example:
- Schools and universities should reopen.
- All leisure activities are permitted
- People should be allowed to return to work. Those over 60 and or with underlying health conditions, and those uncomfortable returning to work, could continue to work at home with support from their employer and government.
- Domestic travel by any means is allowed.
- People at high risk of severe complications by virtue of age (> 60 years) or medical conditions (such as diabetes, cardiovascular disease, cancer or are immunocompromised) should continue to self-isolate and maintain social distance. These people should receive state-funded support and priority care. For example, supermarkets should prioritise all such people for at-home delivery.
- Health professionals should carry out strict hand hygiene and be provided all necessary personal protective equipment.
- High risk communities and groups, with particular focus on rest homes, should be protected from COVID-19 cases or infection and provided government support to do so.
- Gatherings of over 100 people are prevented.
- Encourage improved hand hygiene and exclusion policies for ill workers.
- Border entry is restricted for the near-future to reduce the risk of imported infection.
- Monitor hospitals for overcrowding and limited capacity in intensive care.
- Contact tracing and quarantine of newly identified cases is essential. Resources should be made available to ensure this is adequately carried out.
- Seroprevalence surveys, with PCR, should be considered to assess the proportion of the population who have been exposed to the virus. This would give valuable information about further risks posed to high risk individuals to facilitate their return to the community.
14 April 2020
Expert group suggests way out of lockdown
A specially formed group of local academics, led by public health experts, says New Zealand can and should come out of lockdown, and has proposed a “Plan B” to do that.
The cross-disciplinary group of academics say they understand the rationale for New Zealand’s firm lockdown, but new data and experience of the COVID19 virus signals that it can be managed without the severe health, social and economic effects a lockdown imposes.
Group member Dr Simon Thornley, Senior Lecturer of Epidemiology at University of Auckland, says the lockdown strategy is no longer proportional to the threat posed by COVID-19 to New Zealanders’ health.
“Prolonged lockdown is likely to cause greater harm than the virus to the nations long-term health and well-being, social fabric, economy, and education.
“The real threat of the virus is that it can create more cases than health services can handle. This leads to unnecessary deaths and virus spread. But the risk of this happening is lower in countries such as ours with lower population density, and our health system currently has spare capacity.”
Data shows that a large majority of COVID-19 fatalities have occurred in people due to their comorbidities rather than directly from the virus. Even in Italy only 12% of cases were directly due to COVID.
“If you catch COVID-19 your likelihood of dying is the same as your average likelihood of dying that year anyway. It has been described as squeezing your year’s mortality risk into two weeks,” Thornley says.
“The way we stop the spread of an epidemic virus strain must be proportionate to the threat posed by the infection. The lockdown was appropriate when there was so little data, and when it seemed sensible to try to eliminate it or wait for a vaccine. But the data is now clear – this is not the disaster we feared and prepared for. Elimination of this virus is likely not achievable and is unnecessary. Moreover, elimination will be almost impossible to sustain as the virus is likely to become endemic across the rest of the world, and a vaccine may be years away.”
The group’s Plan B is to end lockdown after the four week period and immediately shift to a risk-based management plan, similar to the Government’s Level 2 format, with the principal aim of preventing stress on the health system.
- Low risk people should be allowed to return to their normal daily activities. For example:
- Schools and universities should reopen.
- All leisure activities are permitted.
- People should be allowed to return to work. Those over 60 and/or with underlying health conditions, and uncomfortable returning to work, could continue to work at home with support from their employer and government.
- Domestic travel by any means allowed.
- People at high risk of severe complications by virtue of age (> 60 years) or medical conditions (such as diabetes, obesity, cardiovascular disease, cancer or immunocompromised) should continue to self-isolate and socially distance. They should receive state-funded support and priority care. e.g prioritised for at-home supermarket delivery.
- Health professionals should carry out strict hand hygiene and be provided all necessary personal protective equipment.
- High risk communities and groups, with particular focus on rest homes, should be protected from COVID-19 cases or infection and provided government support to do so.
- Gatherings of over 100 people are prevented.
- Encourage improved hand hygiene and exclusion policies for ill workers.
- Border entry is restricted for the near-future to reduce the risk of imported infection.
- Monitor hospitals for overcrowding and limited capacity in intensive care.
- Contact tracing and quarantine of newly identified cases is essential. Resources should be made available to ensure this is adequately carried out.
- Seroprevalence surveys, with PCR, should be conducted as soon as possible to assess the proportion of the population who have been exposed to the virus. This would give valuable information about further risks posed to high risk individuals to facilitate their return to the community.
Founding members of the group are:
- Dr Simon Thornley – Senior lecturer of Epidemiology and Biostatistics, The University of Auckland
- Dr Grant Schofield – Professor of Public Health, AUT, Auckland
- Dr Gerhard Sundborn – Senior lecturer of Population and Pacific Health, University of Auckland.
- Dr Grant Morris – Associate Professor of Law, Victoria University of Wellington.
- Dr Ananish Chaudhuri- Professor of Experimental Economics, University of Auckland and Visiting Professor of Public Policy and Decision Making, Harvard University, Massachusetts, USA
- Dr Michael Jackson – Postdoctoral researcher; expertise in biostatistics and biodiscovery, University of Wellington
Contact: Simon Thornley, 021 299 1752 or Mark Blackham, PR: 021 891 042 | https://www.covidplanb.co.nz/
South Korea’s policy of testing, tracing and treating without lockdowns has been widely lauded. Some attribute this to South Korea’s having dealt with previous epidemics such as Sars and Mers. At the roots of South Korea’s success against Covid-19 are a well-funded and efficient system of delivering public services.
https://www.theguardian.com/commentisfree/2020/apr/11/south-korea-beating-coronavirus-citizens-state-testing
Global economic hardship, 1.52 billion students at home, growth in domestic violence and healthcare workers and systems harmed: vicious side-effects for women the United Nations warns.
https://www.theguardian.com/world/2020/apr/11/un-coronavirus-pandemic-gender-inequalities-women
April 11: The people of the city where the first virus was first detected are taking their first cautious steps outside after being confined for three months.
https://www.theguardian.com/world/2020/apr/12/wuhan-celebrates-its-liberation-as-covid-19-lockdown-ends
Data and case – world map. Updated.
https://www.theguardian.com/world/2020/apr/11/coronavirus-world-map-which-countries-have-the-most-cases-and-deaths
April 11: The government faces a chorus of cross-party calls on Sunday for the urgent recall of parliament in “virtual” form as MPs and peers demand the right to hold ministers to account over the escalating coronavirus crisis.
https://www.theguardian.com/world/2020/apr/11/political-parties-demand-recall-parliament-keir-starmer-labour
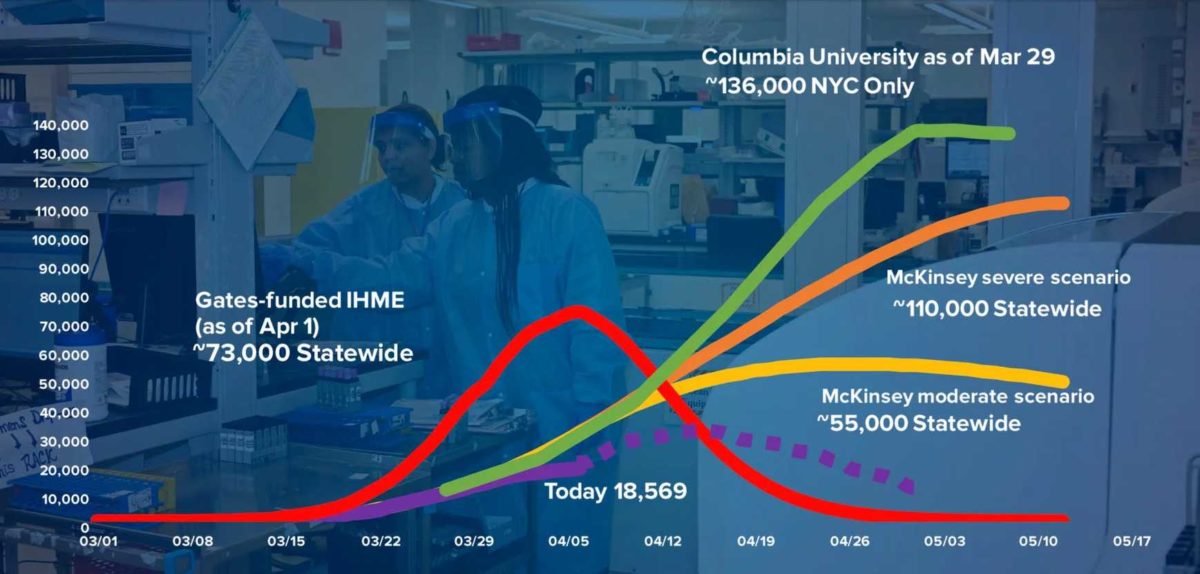
April 10: Officials had estimated that 140,000 hospital beds might be needed to treat coronavirus patients. Only about 18,500 were in use by week’s end.
https://www-nytimes-com.cdn.ampproject.org/c/s/www.nytimes.com/2020/04/10/nyregion/new-york-coronavirus-hospitals.amp.html