22 October 2020
New Zealand has not released any analysis about the negative health impacts of the Covid-19 elimination and lockdown policy.
This is highlighted by studies released in the UK this week which indicates that their lockdowns are responsible for thousands of deaths and new illnesses, principally as a result of delayed cancer diagnoses (see note below).
The only known study of lockdown health impacts in New Zealand was of a Dunedin primary health clinic, where referrals and tests had dropped 100% and 99% respectively. Anecdotal evidence provided to the Covid Plan B group is that referrals and tests may be down across the country by two thirds. Auckland District Health Board is also investigating after four women died during and after pregnancy this year, with three dying since alert level 3 was instituted in late March. Expected numbers of deaths are between 0 and one from previous years.
Evidence provided from affected individuals indicate illnesses and health prognosis have worsened due to delayed tests and treatment. Whether these cases represent a wider problem is not known.
Dr Simon Thornley, spokesman for Covid Plan B, said the Government’s elimination and lockdown policy was based on hope, because little analysis of the downsides of the policy has been carried out.
“If you base your rationale on discredited models and you don’t count impacts, this is not a policy based on evidence.
“This is a policy based on an assumption that the low Covid-19 impact is the result of the lockdown policy. There is no proof of that, and international studies indicate it is unlikely.
“This is also a policy continued on the assumption that there are no negative effects. But firsthand testimony in New Zealand and overseas statistics suggest this is not true. Economic analysis from the government and independent sources indicate that lockdowns are a disproportionate response to Covid-19. The effect on unemployment is now clear, with a 38% rise in adults on the jobseeker benefit since late March. Now, the impact of delayed diagnosis and under treatment of other conditions must be considered.
“We are not even trying to count what the other effects have been on health. We do not know how many people have died, had conditions or prognosis worsen because of the ways lockdown and fear have affected healthcare.
“We call on the Ministry of Health to undertake the same studies we’ve seen in the UK, and to weigh those costs against what they imagine, or count, are the benefits of the elimination strategy,” Simon Thornley says.
– ends
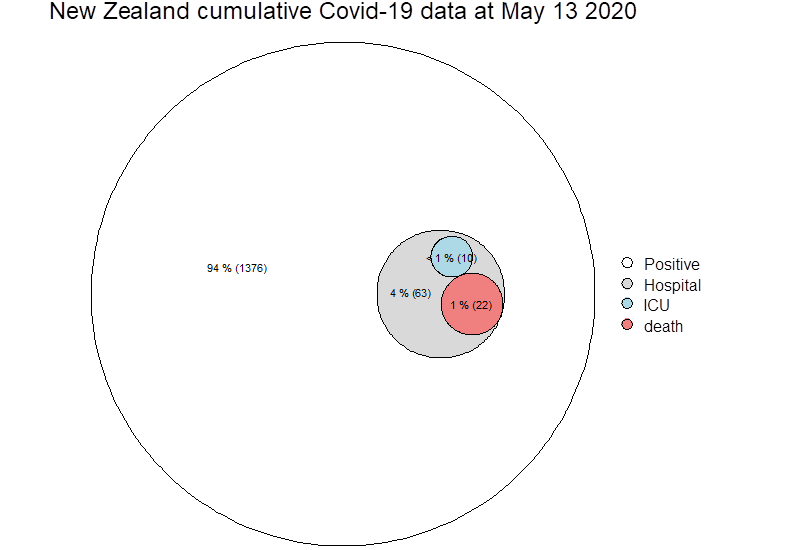
 Zeroing on test positive cases (blue circle above, now below), it is not possible from paper to know how many deaths actually went to ICU, so these cells may not be mutually exclusive…
Zeroing on test positive cases (blue circle above, now below), it is not possible from paper to know how many deaths actually went to ICU, so these cells may not be mutually exclusive…