31 August 2020
A supporter has sent us a massive amount of Covid research. We have not checked every link, so use with caution and discretion. With their permission, we reprint it below.
But remember that it is not an absence of science that caused the international panic, and still causes it in New Zealand. The evidence is abundant and clear.
Yet mainstream scientists, politicians, media, commentators, remain obsessed with the goal of elimination, the use of lockdowns, and a fear of death from Covid over more dangerous diseases.
So there are deeply rooted psychological and social drivers behind their panic. Throwing facts at them won’t change their mind instantly. It may even be counter-productive. We have to ride this out until people come to their senses in their own way and time. We can help them change their minds by being persistent, civil, generous and succinct.
—
There are a few main reasons to be optimistic we should end lockdowns and get back to normal.
1) We know who this coronavirus affects. The median age of death in almost all countries is over 80 with multiple existing conditions. We are failing to protect old people and are locking up the young and imposing social distancing when they have no risk of death. We can protect the vulnerable more intelligently.
2) Most people have immunity due to cross reactivity and cross immunization. The human immune system is not completely helpless against this virus.
3) Herd immunity levels are much lower than people think and the virus appears to follow a Gompertz curve, which correctly anticipates the virus fizzling out
WHY LOCKDOWNS ARE TERRIBLE IDEAS
Those in favor of lockdown present a false dichotomy. Either we have a hard lockdown or we let the virus rip and kill everyone. That is hardly the case. Lockdowns and business closures are a sledgehammer that had no precedent in history and are not the way we have ever treated any virus or pandemic before. The costs are out of all proportion to the benefits. Many other strategies would be far better.
Here is a great case against lockdowns
How a Free Society Deals with Pandemics, According to Legendary Epidemiologist and Smallpox Eradicator Donald Henderson
https://www.aier.org/article/how-a-free-society-deals-with-pandemics-according-to-legendary-epidemiologist-and-smallpox-eradicator-donald-henderson/
It concluded with this important paper
http://www.upmc-biosecurity.org/website/resources/publications/2006/2006-09-15-diseasemitigationcontrolpandemicflu.html
There are no historical observations or scientific studies that support the confinement by quarantine of groups of possibly infected people for extended periods in order to slow the spread of influenza. A World Health Organization (WHO) Writing Group, after reviewing the literature and considering contemporary international experience, concluded that “forced isolation and quarantine are ineffective and impractical.”2 Despite this recommendation by experts, mandatory large-scale quarantine continues to be considered as an option by some authorities and government officials.35,43
The interest in quarantine reflects the views and conditions prevalent more than 50 years ago, when much less was known about the epidemiology of infectious diseases and when there was far less international and domestic travel in a less densely populated world. It is difficult to identify circumstances in the past half-century when large-scale quarantine has been effectively used in the control of any disease.
The negative consequences of large-scale quarantine are so extreme (forced confinement of sick people with the well; complete restriction of movement of large populations; difficulty in getting critical supplies, medicines, and food to people inside the quarantine zone) that this mitigation measure should be eliminated from serious consideration.
No country had lockdowns in their playbook.
For example, Canada’s pandemic guidelines concluded that restrictions on movement were “impractical if not impossible.”
https://www.canada.ca/en/public-health/services/flu-influenza/canadian-pandemic-influenza-preparedness-planning-guidance-health-sector/table-of-contents.html
Also, according to the Wall Street Journal, “The U.S. Centers for Disease Control and Prevention, in its 2017 community mitigation guidelines for pandemic flu, didn’t recommend stay-at-home orders or closing nonessential businesses even for a flu as severe as the one a century ago.”
It was never part of the US response
https://pubmed.ncbi.nlm.nih.gov/17238820/
Lockdowns were never part of the WHO standard responses for pandemics
(you can read here all their policies and how they rated the evidence for various measures)
https://www.who.int/influenza/publications/public_health_measures/publication/en/
Most Asian countries like Taiwan, Japan and South Korea didn’t have hard lockdowns and had far better experiences than the European countries that did. Those who are sick are not sent home to infect family members and are separated, which is the exact opposite of European lockdowns.
https://www.vox.com/2020/4/28/21238456/centralized-isolation-coronavirus-hong-kong-korea
Here is a very good read on the arguments against lockdowns. In most European countries, cases were already falling before the lockdowns as people were voluntarily taking preventive measures: social distancing, hand washing, wearing masks.
https://www.thepublicdiscourse.com/2020/04/62837/
Here is a study in The Lancet showing lockdowns had no effect. The primary factors explaining deaths are obesity and age structure
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(20)30208-X/fulltext
And another detailed study showing the virus behaved the same everywhere regardless of policy
https://t.co/KwVF9UG1N2?amp=1
Same is true on a county by county basis in the US. Whether a county had a lockdown has no effect on Covid-19 deaths; a non-effect that persists over time.
https://ideas.repec.org/p/wai/econwp/20-06.html
One of the biggest determinant of deaths from Covid related to the share of the population that was over 80, not to lockdowns
https://marketmonetarist.com/2020/04/20/one-factor-explains-most-of-the-differences-in-covid19-deaths-across-countries/
The other explainers are percentage of the population with hypertension
https://www.weforum.org/agenda/2020/05/this-is-why-people-with-obesity-are-more-likely-to-die-from-coronavirus
and percentage of population with obesity/diabetes
https://www.independent.co.uk/news/uk/home-news/coronavirus-obesity-death-rates-uk-global-who-a9612626.html
Here are more studies showing that the deaths were falling before the lockdowns were imposed
https://www.medrxiv.org/content/10.1101/2020.04.24.20078717v1
and https://www.econstor.eu/handle/10419/216971
and https://www.spectator.co.uk/article/new-study-shows-covid-infections-were-falling-before-lockdown
The decline in infections started before Germany even instituted lockdowns
https://www.sciencedirect.com/science/article/pii/S0925753520303210
Bloomberg also found little correlation between severity of measures and death rates.
https://www.bloomberg.com/graphics/2020-opinion-coronavirus-europe-lockdown-excess-deaths-recession/
and here is a similar piece in the WSJ by economists.
https://www.wsj.com/articles/do-lockdowns-save-many-lives-is-most-places-the-data-say-no-11587930911
The other issue is there are tradeoffs to the current policy.
More Than Half of US Business Closures Permanent, Yelp Says
https://www.bloomberg.com/news/articles/2020-07-22/more-than-half-of-u-s-business-closures-permanent-yelp-says
As the Telegraph reported, the consequences for poverty and children is horrific.
https://www.telegraph.co.uk/global-health/science-and-disease/unicef-warns-lockdown-could-kill-covid-19-model-predicts-12/
Furthermore, there is good reason to believe that lockdowns increased deaths of the vulnerable and elderly.
https://www.lboro.ac.uk/news-events/news/2020/july/new-approach-to-recording-covid-deaths/
This is true in much of the world. Here is a study looking at how lockdowns drove excess deaths for non-Covid illnesses
https://www.researchgate.net/publication/343775235_Evaluation_of_the_virulence_of_SARS-CoV-2_in_France_from_all-cause_mortality_1946-2020
Denver doctors may have found the answer to a pandemic mystery: What happened to all the heart attacks?
https://coloradosun.com/2020/08/17/denver-coronavirus-deaths-heart-attack/
Stauffer and his colleagues found that the number of people in Denver who died of cardiac arrests at home in the two weeks following the statewide stay-at-home order was greater than the total number of people who died of COVID-19 in the city during that time.
New cancer diagnoses fell sharply as the coronavirus pandemic first hit
https://www.statnews.com/2020/08/04/new-cancer-diagnoses-fell-sharply-after-coronavirus/
Almost all diagnoeses collapsed in the UK.
https://www.ippr.org/blog/the-hidden-cost-of-covid-19-on-the-nhs
And same was true for heart attacks and strokes.
Analysis of NHS data reveals the deadly consequences of the government’s messaging to ‘stay at home, save lives, protect the NHS.’ During the lockdown, there was a near 50 per cent decline in admissions for heart attacks. The risks of Covid-19 outweighed the risk of seeking NHS care despite worsening symptoms for many people: 40 per cent more people died from lower-risk treatable heart attacks than usual. For strokes, the situation is further exacerbated by living alone and not having visitors as 98 per cent of emergency calls for strokes are made by someone else.
Covid is not the only illness in the world.
Tuberculosis. From the NY Times.
https://www.nytimes.com/2020/08/03/health/coronavirus-tuberculosis-aids-malaria.html
Tuberculosis kills 1.5 million people each year. Lockdowns and supply-chain disruptions threaten progress against the disease as well as H.I.V. and malaria.
According to one estimate, a three-month lockdown across different parts of the world and a gradual return to normal over 10 months could result in an additional 6.3 million cases of tuberculosis and 1.4 million deaths from it.
A six-month disruption of antiretroviral therapy may lead to more than 500,000 additional deaths from illnesses related to H.I.V., according to the W.H.O. Another model by the W.H.O. predicted that in the worst-case scenario, deaths from malaria could double to 770,000 per year.
Many epidemiologists have been completely opposed to government plans and have in fact been right. Only pro-lockdown scientists are amplified. Here is a good read on “the science.”
https://www.spectator.com.au/2020/07/the-covid-conundrum/
Here is Sunetra Gupta of Oxford
https://www.theguardian.com/world/2020/jun/05/the-costs-are-too-high-the-scientist-who-wants-lockdown-lifted-faster-sunetra-gupta
https://unherd.com/2020/05/oxford-doubles-down-sunetra-gupta-interview/
and Martin Kuldorff, a Harvard epidemiologist who has been ignored
and https://www.linkedin.com/pulse/covid-19-counter-measures-should-age-specific-martin-kulldorff/
https://www.spectator.co.uk/article/herd-immunity-is-still-key-in-the-fight-against-covid-19
HOW DID WE GET LOCKDOWNS?
Public pressure, not science.
https://twitter.com/BallouxFrancois/status/1298735505543225346?s=20
The only epidemiologists advocating for lockdowns were at Imperial College. The Imperial College model predicted that even with mitigation measures, over a million would die in the US and 250,000 would die in the UK. https://www.cato.org/blog/how-one-model-simulated-22-million-us-deaths-covid-19
These estimates were wildly off by a factor of 10. It should be no surprise. The same team at Imperial forecast 200 million would die in 2005 of Bird Flu but only 43 people died from it that year. https://www.theguardian.com/world/2005/sep/30/birdflu.jamessturcke
Why did the west lock down even though the scientific advisers in the UK, Italy, Sweden and other countries were against them initially?
Public pressure is the answer. For example, here is the article that was viewed 40 million times, even though it wasn’t written by an empidemiologist but rather by a Silicon Valley “growth hacker” whose only claim to fame is writing a book on Star Wars and speaking at TEDx. You cann’t make this up. His other posts were read 60 million times encouraging lockdowns and social restrictions.
https://medium.com/@tomaspueyo/coronavirus-act-today-or-people-will-die-f4d3d9cd99ca
The frenzy of social media played a big role, not proper epidemiological practice.
As this well researched piece shows, the main driver of lockdowns was political leaders imitating each other rather than sound planning or advice.
https://www.pnas.org/content/early/2020/08/10/2010625117
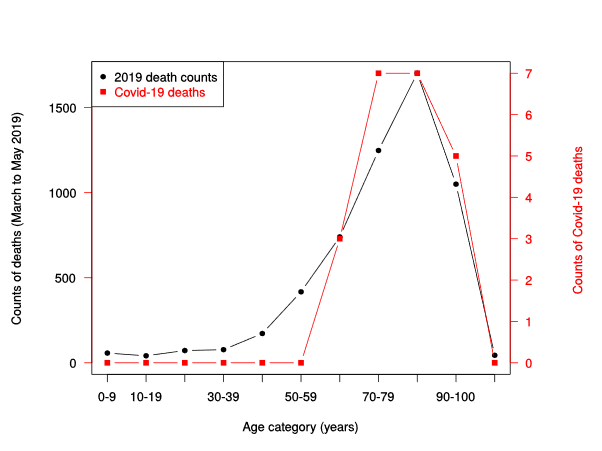
THE VIRUS IS NOT AT ALL DEADLY FOR THOSE UNDER 50
The virus is not at all deadly to younger people. Here are death breakdowns by age group in the US and Europe
https://twitter.com/MLevitt_NP2013/status/1286177208583815168?s=20
and another visualization
https://twitter.com/kylamb8/status/1287952340822175744/photo/1
And from the Oxford for Evidence Based Medicine (scroll to bottom)
https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates/
Here is the link to all the studies on infection fatality rates for Covid. The evidence is overwhelming that it is much lower than the initial dire estimates.
https://swprs.org/studies-on-covid-19-lethality/
From one paper looking at Infection fatality rates by age summarized it well.
“The estimated IFR is close to zero for younger adults but rises exponentially with age, reaching about 0.3% for ages 50-59, 1.3% for ages 60-69, 4% for ages 70-79, 10% for ages 80-89.”
https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v3
The median age for death in most countries is over 80 and the average person has multiple pre-existing conditions
In Italy the median age was over 80 and 96% of people had existing conditions
https://www.statista.com/statistics/1105061/coronavirus-deaths-by-region-in-italy/
https://www.bloomberg.com/news/articles/2020-05-26/italy-says-96-of-virus-fatalities-suffered-from-other-illnesses
Spain showed exactly the same pattern
https://www.statista.com/statistics/1105596/covid-19-mortality-rate-by-age-group-in-spain-march/
Ireland is the same
https://www.irishexaminer.com/breakingnews/ireland/majority-of-those-who-died-with-covid-19-had-underlying-condition-figures-reveal-1002419.html
US – Median death age from Covid in the US was 80 years.
https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6928e1-H.pdf
That is slightly above the average life expectancy overall
https://www.cdc.gov/nchs/data/hus/2018/fig01.pdf
In many countries the median age of death is above life expectancy, i.e. people had already lived longer than the average person.
https://www.dailymail.co.uk/news/article-8470843/The-average-Covid-19-victim-OLDER-age-people-usually-die-Scotland.html
Population-level COVID-19 mortality risk for non-elderly individuals overall and for non-elderly individuals without underlying diseases in pandemic epicenters
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7327471/
The COVID-19 mortality rate in people <65 years old during the period of fatalities from the epidemic was equivalent to the mortality rate from driving between 4 and 82 miles per day for 13 countries and 5 states, and was higher (equivalent to the mortality rate from driving 106–483 miles per day) for 8 other states and the UK. People <65 years old without underlying predisposing conditions accounted for only 0.7–3.6% of all COVID-19 deaths in France, Italy, Netherlands, Sweden, Georgia, and New York City and 17.7% in Mexico.
People <65 years old have very small risks of COVID-19 death even in pandemic epicenters and deaths for people <65 years without underlying predisposing conditions are remarkably uncommon. Strategies focusing specifically on protecting high-risk elderly individuals should be considered in managing the pandemic.
Most people had hypertension as a co-morbidity
A key point is that people with hypertension have a lower life expectancy with or without Covid
https://www.ahajournals.org/doi/10.1161/01.hyp.0000173433.67426.9b
Irrespective of sex 50-year-old hypertensives compared with normotensives had a shorter life expectancy a shorter life expectancy free of cardiovascular disease myocardial infarction and stroke and a longer life expectancy lived with these diseases. Normotensive men (22% of men) survived 7.2 years (95% confidence interval, 5.6 to 9.0) longer without cardiovascular disease compared with hypertensives and spent 2.1 (0.9 to 3.4) fewer years of life with cardiovascular disease. Similar differences were observed in women…. Compared with hypertensives total life expectancy was 5.1 and 4.9 years longer for normotensive men and women respectively. Increased blood pressure in adulthood is associated with large reductions in life expectancy and more years lived with cardiovascular disease. This effect is larger than estimated previously and affects both sexes similarly. Our findings underline the tremendous importance of preventing high blood pressure and its consequences in the population.
The same is true for diabetes.
https://care.diabetesjournals.org/content/40/3/338
https://dlife.com/life-expectancy-prediabetes-type1-type2-type3-diabetes/
According to the reports of Journal of American Medical Association (JAMA); men with type 1 diabetes have a shortened lifespan of 11 years than normal men. Women with the condition have their lives cut short by 13 years.
A 2010 report by the Diabetes UK claims that type 2 diabetes reduces the lifespan by 10 years. A 2012 Canadian study claimed that women aged over 55 years with type 2 diabetes lost on an average of 6 years while men lost 5.
The probability of dying under 65 without co-morbidities is extremely low to non-existent.
It is far more sensible to protect the vulnerable than close society.
CHILDREN DO NOT SPREAD THE VIRUS AND ARE NOT AT RISK
Sweden kept their schools open and not a single child died from Covid of over 1.8 million kids.
https://www.reuters.com/article/us-health-coronavirus-sweden-schools-idUSKCN24G2IS
Closure or not of schools has had little if any impact on the number of laboratory confirmed cases in school aged children in Finland and Sweden.
https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/c/covid-19-in-schoolchildren/
In fact, children are more likely to be hit by lightning than die from Covid.
https://www.express.co.uk/news/uk/1293683/coronavirus-news-schools-reopening-lockdown-end-children-latest
Children are more likely to die from flu than Covid.
https://twitter.com/gummibear737/status/1291399160827125762
No transmission from children in Greece. Transmission dynamics of SARS‐CoV‐2 within families with children in Greece: a study of 23 clusters
https://onlinelibrary.wiley.com/doi/abs/10.1002/jmv.26394
COVID-19 Transmission and Children: The Child Is Not to Blame
https://pediatrics.aappublications.org/content/146/2/e2020004879
No evidence of secondary transmission of COVID-19 from children attending school in Ireland 2020
https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.21.2000903#metrics_content
German study shows low coronavirus infection rate in schools
https://nationalpost.com/pmn/health-pmn/german-study-shows-low-coronavirus-infection-rate-in-schools
Children are not COVID-19 super spreaders: time to go back to school
https://adc.bmj.com/content/105/7/618.info
The Royal College of Paediatricans and Child Health review of the evidence
https://www.rcpch.ac.uk/resources/covid-19-research-evidence-summaries
A CDC showing very limited transmission in childcare settings
https://www.cdc.gov/mmwr/volumes/69/wr/mm6934e2.htm?s_cid=mm6934e2_w
PUBLIC POLICY RESPONSE DUE TO AGE DIFFERENCES
Here is a good read from a Harvard professor of epidemiology.
Delaying herd immunity is costing lives. The current lockdown is protecting the healthy instead of the vulnerable.
https://www.spiked-online.com/2020/04/29/delaying-herd-immunity-is-costing-lives/
He also wrote a very good piece on the proper response. Given the age differences in risk, policy responses should be age specific
https://www.linkedin.com/pulse/covid-19-counter-measures-should-age-specific-martin-kulldorff/
Strategies targeted by age are likely to be much more useful at reaching herd immunity with less damage
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0236237
ELDERLY ARE MOST VULNERABLE, 50-60% OF ALL DEATHS WERE CARE HOME DEATHS
In most countries between 50-60% of deaths from Covid are from care homes. In some countries and states it is as high as 80%. What is extraordinary, though, is that this is largely a self-inflicted wound. Many infected old people were sent away from hospitals to care homes to infect others. This is true in the UK, NY and California.
While Covid deaths are horrible, it is worth considering what life expectancy without Covid would be in care homes.
Even without Covid, life expectancy is extremely short in care homes.
https://www.geripal.org/2010/08/length-of-stay-in-nursing-homes-at-end.html
https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1532-5415.2010.03005.x
The length of stay data were striking:
- the median length of stay in a nursing home before death was 5 months
- 65% died within 1 year of nursing home admission
- 53% died within 6 months of nursing home admission
The finding of median death in nursing homes being less than one year is confirmed in other studies. Median death is under a year.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3050554/
and
https://academic.oup.com/psychsocgerontology/article/55/3/S152/607093
Caregivers who institutionalize their relatives are substantially more likely to become bereaved than those whose relatives continue to reside at home. The zero-order odds of patient death more than double following admission to a nursing home
This is by far the best site on all issues relating to care homes internationally. It shows percentage of all Covid deaths are 50-60% for almost all countries.
https://ltccovid.org/
Here is their main report with extensive data by country and 50-60% of deaths on average
https://ltccovid.org/international-reports-on-covid-19-and-long-term-care/
42% Of U.S. Deaths Are From 0.6% Of The Population in Care homes
https://www.forbes.com/sites/theapothecary/2020/05/26/nursing-homes-assisted-living-facilities-0-6-of-the-u-s-population-43-of-u-s-covid-19-deaths/#1b1838e274cd
The Real Pandemic Was a Nursing Home Problem from The American Institute for Economic Research
https://www.aier.org/article/the-real-pandemic-was-a-nursing-home-problem/
Some countries and states have 70-80% of all deaths in care homes.
Canada 82%
https://www.thestar.com/politics/federal/2020/05/07/82-of-canadas-covid-19-deaths-have-been-in-long-term-care.html
80% in Northern Ireland
https://www.bbc.com/news/uk-northern-ireland-52774149
Here is NJ at 76%
https://www.njherald.com/news/20200510/long-term-care-deaths-now-76-of-countyrsquos-covid-total
70% in Ohio
https://www.cleveland.com/coronavirus/2020/05/with-1442-dead-nursing-homes-account-for-70-of-ohios-coronavirus-deaths.html
https://www.msn.com/en-us/health/medical/ohio-reports-1860-nursing-home-patients-now-dead-with-coronavirus/ar-BB15DmSG
70% in Pennsylvania
https://pittsburgh.cbslocal.com/2020/05/05/pennsylvania-nursing-homes-coronavirus/
70% in Arizona
https://www.insurancejournal.com/news/west/2020/06/01/570598.htm
70% Florida
https://www.miamiherald.com/news/coronavirus/article243096941.html
Over the most recent week, elders living in long-term care facilities accounted for 7 in 10 Florida deaths resulting from the coronavirus, as the pandemic increasingly became a scourge of the old and frail.
Here is data from US nursing homes regarding deaths
https://www.wsj.com/articles/coronavirus-deaths-in-u-s-nursing-long-term-care-facilities-top-50-000-11592306919
This is an extraordinary resource that shows care home deaths in the US.
https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg
70% in Sweden. Sweden’s complete failure to protect elderly care homes that is the problem, not the lack of lockdown.
“Upwards of 70 percent of the Covid19 death toll in Sweden has been people in elderly care services (as of mid-May 2020).”
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3609493
This is a very good read on the problems of Swedish care homes.
https://ltccovid.org/2020/05/08/covid-19-reveals-serious-problems-in-swedish-long-term-care/
It is likely care home deaths are understated and hospital overstated.
15% of hospital deaths in the UK were actually care home deaths according to the ONS
https://www.standard.co.uk/news/health/care-home-deaths-ons-covid19-latest-figures-a4441416.html
“Of the Covid-related deaths, 9,039 occurred within a care home, while a further 3,444 occurred within a hospital. Of all hospital deaths involving Covid-19 during this period, 14.6 per cent were accounted for by care-home residents.”
It is astonishing how people still obsess about everyone getting it and dying, when the danger is care homes. There is still no coordinated response to protect them.
POLITICIANS ENGINEERING CARE HOME DEATHS THROUGH BAD POLICY
Look at California’s insane policy. This is from California from May 4th, not early on. They already knew about care home transmission.
https://www.mercurynews.com/2020/05/04/california-offers-senior-care-facilities-contracts-to-accept-covid-19-patients/
https://www.mercurynews.com/2020/05/06/editorial-newsom-falters-as-covid-19-nursing-home-cases-soar/
This is packed with links.
https://pjmedia.com/news-and-politics/victoria-taft/2020/05/27/californias-covid-nursing-home-death-rate-cover-up-is-imploding-n433703
Here was NY. https://nypost.com/2020/04/26/cuomo-doubles-down-on-sending-coronavirus-patients-to-nursing-homes/
New Jersey, Pennsylvania and the Northaast
https://www.buckscountycouriertimes.com/news/20200501/states-ordered-nursing-homes-to-take-covid-19-residents-thousands-died-how-it-happened
and the UK
https://www.dailymail.co.uk/news/article-8302039/Hospitals-probed-sending-elderly-care-homes-despite-KNOWING-coronavirus.html
https://www.telegraph.co.uk/news/2020/04/15/discharging-coronavirus-patients-care-homes-madness-government/
The only correct historical analogy is the Siege of Caffa where Tartars threw infected bodies of the dead over city walls to spread the disease
https://twitter.com/afneil/status/1260264151429062657 [twitter.com]
and
http://birthstory.net/history/the-black-plague-and-the-siege-of-caffa/
WHY HERD IMMUNITY THRESHOLDS IN REALITY ARE MUCH LOWER THAN IN THEORY
The short and simple reason why herd immunity is reached at much lower levels than people think is that populations are not homogenous i.e. we have different age groups with different susceptibilities, and we all don’t mix randomly, i.e. most people live boring lives and see the same people every day. Simply put, heterogeneity and non-random mixing massively reduce the threshold for herd immunity.
Here is a good accessible explanation of why herd immunity levels are much lower than expected for many diseases
https://reason.com/2020/05/15/whats-the-herd-immunity-threshold-for-the-covid-19-coronavirus/
Here is a long blog post with links to studies on how the herd immunity threshold is lower than people think.
https://judithcurry.com/2020/07/27/why-herd-immunity-to-covid-19-is-reached-much-earlier-than-thought-update/
And a slightly more technical explanation.
https://wattsupwiththat.com/2020/05/11/why-herd-immunity-to-covid-19-is-reached-much-earlier-than-thought/
Here is an introduction to the question of why estimating herd immunity isn’t straightforward or high like the media argue.
https://www.quantamagazine.org/the-tricky-math-of-covid-19-herd-immunity-20200630/
And a discussion of why immunity levels are lower than classically assumed
https://www.webmd.com/lung/news/20200626/herd-immunity-threshold-could-be-as-low-as-43-percent
and https://covidplanningtools.com/are-we-closer-to-herd-immunity-than-the-experts-say/
Here is a paper noting that Herd Immunity Thresholds are much lower in Sweden.
https://www.medrxiv.org/content/10.1101/2020.05.19.20104596v1
Early estimates of HIT for Covid-19 were based on this simplistic homogeneous approach, yielding high HIT values that have since been revised downwards with more sophisticated network modelling taking account of R0 heterogeneity and with reference to the low HIT found from serological sampling in Stockholm County.
Here is an academic paper on why Covid will have lower herd immunity thresholds
https://www.medrxiv.org/content/10.1101/2020.04.27.20081893v3
The disease-induced herd immunity level for Covid-19 is substantially lower than the classical herd immunity level
https://arxiv.org/abs/2005.03085
Heterogenous transmission is likely why we have more cases with lower deaths. The virus spreads in less susceptible people
http://math.cmu.edu/~wes/covid.html
Here is a broader read on heterogeneity of populations and the effectiveness of vaccines
https://mbio.asm.org/content/8/6/e00796-17.abstract
The reason care homes are so vulnerable is that populations are not heterogenous.
https://twitter.com/bansallab/status/1258872610210877442?s=20
and paper
https://t.co/gabCWUtNub?amp=1
Here is a discussion of the role of non-random mixing from a few months ago, which turns out to be spot on with current death rates.
https://www.haaretz.com/israel-news/.premium.MAGAZINE-israeli-expert-trump-is-right-about-covid-19-who-is-wrong-1.8691031
Much lower effective herd immunization thresholds fit what we see every year with flus, even bad ones.
According to the WHO about 15% of people get flu a year, not 80%.
https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/data-and-statistics
According to the CDC about 3-11%% of the population gets the flue any year, and that includes asymptomatic people
https://www.cdc.gov/flu/about/keyfacts.htm
How Many People Get Sick with Flu Every Year?
A 2018 CDC study published in Clinical Infectious Diseasesexternal icon looked at the percentage of the U.S. population who were sickened by flu using two different methods and compared the findings. Both methods had similar findings, which suggested that on average, about 8% of the U.S. population gets sick from flu each season, with a range of between 3% and 11%, depending on the season.
Why is the 3% to 11% estimate different from the previously cited 5% to 20% range?
The commonly cited 5% to 20% estimate was based on a study that examined both symptomatic and asymptomatic influenza illness, which means it also looked at people who may have had the flu but never knew it because they didn’t have any symptoms. The 3% to 11% range is an estimate of the proportion of people who have symptomatic flu illness.
The last pandemic was H1N1 and that peaked at 24% of the global population during the first year. That is one the very high end.
https://www.cidrap.umn.edu/news-perspective/2013/01/study-puts-global-2009-pandemic-h1n1-infection-rate-24
These numbers are, overall, moderately higher than estimates the US Centers for Disease Control and Prevention (CDC) made for the impact of the pandemic in the United States from April 2009 to April 2010. The agency estimated that 61 million Americans had been infected, or about 19.8% of the 2010 population of 308.7 million, as compared with 24% in the WHO study. The CDC said the total could have been anywhere from 43 million to 89 million, with 61 million as the midlevel estimate.
If you want further background reading, here is a terrific overview of herd immunity in a scientific paper.
https://academic.oup.com/cid/article/52/7/911/299077
MOST PEOPLE HAVE IMMUNITY AND A DEFENSE RESPONSE
CROSS REACTIVITY AND CROSS IMMUNIZATION
A study of patients and their families shows that an unexpected six out of eight family members who caught the virus at home had T cell responses but no detectable antibodies.
Intrafamilial Exposure to SARS-CoV-2 Induces Cellular Immune Response without Seroconversion
https://www.medrxiv.org/content/10.1101/2020.06.21.20132449v1
Important peer-reviewed paper in Nature about the likely immunity to COVID-19 conferred by T cells
‘SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls‘ –
Here is a paper on cross reactivity in Cell journal indicating 40-50%
https://www.sciencedirect.com/science/article/pii/S0092867420306103
Here is a study done in Sweden showing 30% of blood donors had T-cell responses
https://news.ki.se/immunity-to-covid-19-is-probably-higher-than-tests-have-shown
and a very good piece explaining cross reactivity and why kids don’t get it
https://academic.oup.com/jid/advance-article/doi/10.1093/infdis/jiaa185/5820656
and another
https://www.tandfonline.com/doi/full/10.1080/21645515.2020.1740560
and another
https://www.medrxiv.org/content/10.1101/2020.04.17.20061440v1
and another paper T-cell response to #SARSCoV2 was observed in 81% of uninfected individuals. This immune response was caused by prior exposure to ‘common cold’ coronaviruses.
https://twitter.com/BallouxFrancois/status/1277338436878381063
Here is a brief discussion of another paper
https://twitter.com/davidrliu/status/1243377007016251400?s=20
the paper
https://t.co/SM8vcWcGxp?amp=1
And another on SARS-1 providing cross reactivity
https://twitter.com/BallouxFrancois/status/1266265084143087628?s=20
paper https://t.co/Izyx1Hf1Ny?amp=1
Here is a long thread with links on the issue.
https://twitter.com/AskeladdenTX/status/1266479519789191168?s=20
Cross reactivity is likely to come from other vaccines people already have.
There is a strong relationship between MMR vaccine and age-stratified COVID fatality rates. Here is the study. https://t.co/7XLCguml9a
MMR Vaccine Appears to Confer Strong Protection from COVID-19: Few Deaths from SARS-CoV-2 in Highly Vaccinated Populations
https://www.researchgate.net/publication/341354165_MMR_Vaccine_Appears_to_Confer_Strong_Protection_from_COVID-19_Few_Deaths_from_SARS-CoV-2_in_Highly_Vaccinated_Populations
Karl Friston: up to 80% not even susceptible to Covid-19
https://unherd.com/2020/06/karl-friston-up-to-80-not-even-susceptible-to-covid-19/
https://www.theguardian.com/world/2020/may/31/covid-19-expert-karl-friston-germany-may-have-more-immunological-dark-matter
Here is good summary of the issue of existing immunity and cross-reactivity for non-scientists
https://www.conservativereview.com/news/horowitz-bombshell-study-half-uninfected-population-already-partially-immune/
and
https://www.theguardian.com/commentisfree/2020/jun/25/viral-immunologist-antibody-tests-covid-19-immuity-coronavirus
In this interview, Sunetra Gupta from Oxford University hits on cross reactivity but doesn’t go into technical details.
https://unherd.com/2020/05/oxford-doubles-down-sunetra-gupta-interview/
As she sees it, the antibody studies, although useful, do not indicate the true level of exposure or level of immunity. First, many of the antibody tests are “extremely unreliable” and rely on hard-to-achieve representative groups. But more important, many people who have been exposed to the virus will have other kinds of immunity that don’t show up on antibody tests — either for genetic reasons or the result of pre-existing immunities to related coronaviruses such as the common cold.
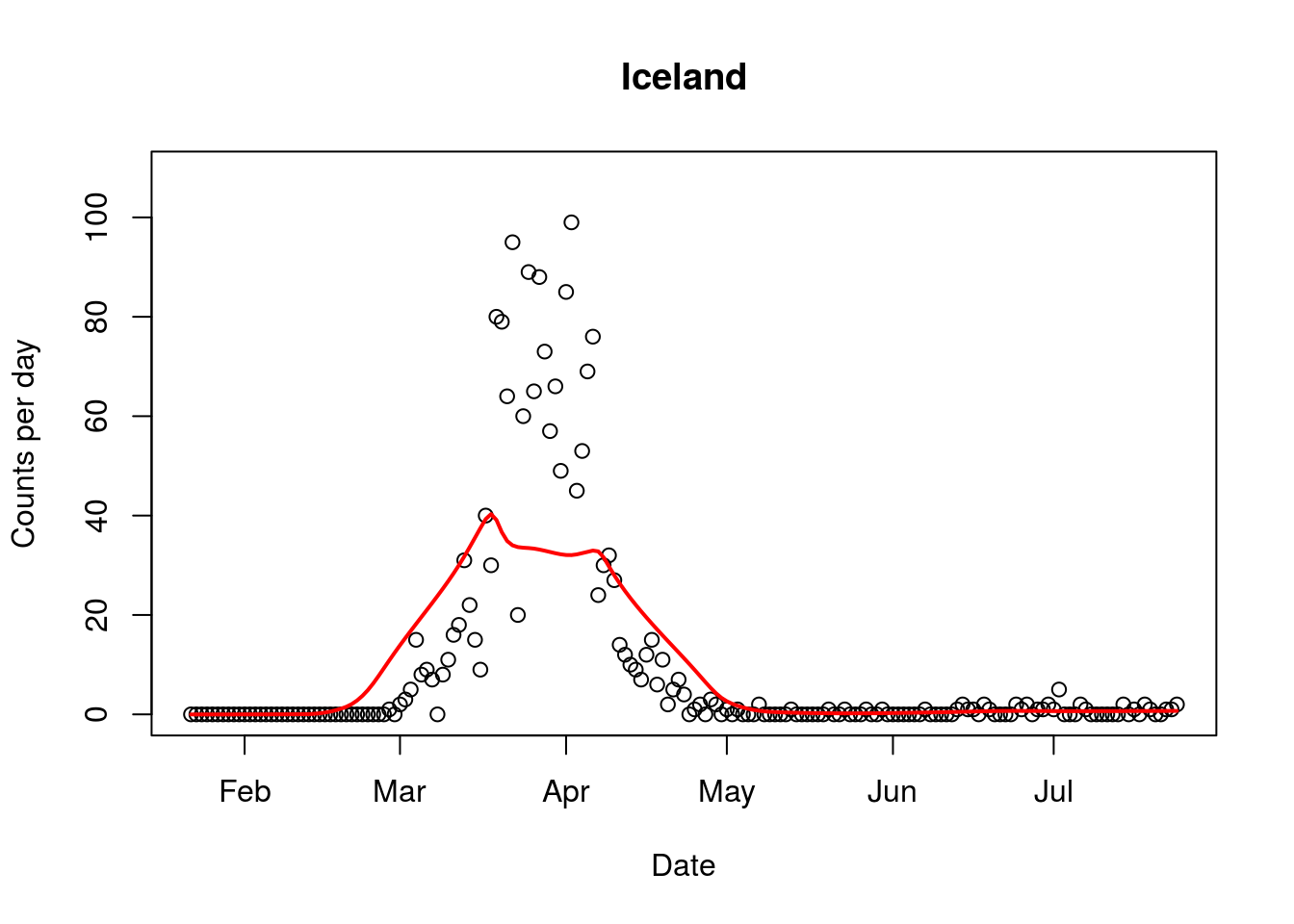
THE VIRUS NATURALLY FIZZLES OUT
MOST STATES/COUNTRIES FOLLOW THE GOMPERTZ CURVE
We know that the virus naturally fizzles out because we have Sweden and Manaus in Brazil and other natural experiments where there were no lockdowns. In Manaus, there were no distancing measures either, and the virus fizzled out.
https://www.washingtonpost.com/world/the_americas/brazil-coronavirus-manaus-herd-immunity/2020/08/23/0eccda40-d80e-11ea-930e-d88518c57dcc_story.html
and Sweden you can see deaths and ICU cases are in the single digits
https://experience.arcgis.com/experience/09f821667ce64bf7be6f9f87457ed9aa
All of this explains stories like this where experts wonder about why the virus fizzles out at a certain point
Curious pattern in coronavirus infection rate emerges, hinting it can ‘burn out’ at a certain point
https://www.news.com.au/technology/science/curious-pattern-in-coronavirus-infection-rate-emerges-hinting-it-can-burn-out-at-a-certain-point/news-story/d83445bad2f312f8a921b6e19b4fb625
Farr’s law explains why viruses don’t grow exponentially and infect everyone.
https://www.cebm.net/covid-19/covid-19-william-farrs-way-out-of-the-pandemic/
Nobel prize winner Michael Levitt has written a paper on the math behind how viruses fizzle out, which fits much lower herd immunity levels
https://www.medrxiv.org/content/10.1101/2020.06.26.20140814v2
Here is an explanation in plain English.
https://www.news-medical.net/news/20200629/Stanfords-Nobel-Laureate-develops-a-prediction-model-for-SARS-CoV-2.aspx
Interestingly, there were a few papers from China and Spain (in Spanish, but you can use Google or Bing translator) that correctly predicted the peaks and end of the virus and number of deaths using Gompertz curves as far back as March
https://www.startpage.com/do/dsearch?query=gompertz+virus&cat=web&pl=ext-ff&language=english&extVersion=1.3.0
There are specific reasons why the virus follows a Gompertz function
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7273247/
While some countries look like they’re having second waves or not following the Gompertz curve, the truth is they are. For example, Brazil is actually many big cities that have their own curves. https://twitter.com/gummibear737/status/1286291840715685889 and https://twitter.com/gummibear737/status/1286291842431156226?s=20
And deaths are following the Gompertz curve by city, so see Rio, for example.
https://twitter.com/ciquelero/status/1286297800687353856/photo/2
All European cases are now close to zero and all curves look the same by country
https://twitter.com/FatEmperor/status/1295654821744332800/photo/2
and for Europe as a whole
https://twitter.com/FrontMkt/status/1296439698907373569/photo/1
UK is at zero and looks exactly the same
https://twitter.com/AlistairHaimes/status/1296477016531886080?s=20
The same is true in the US. Early states like NY and NJ have almost no deaths and look like Europe. Later states that had no first wave looked like Eastern Europe. It is now peaking and turning down.
TREATMENT HAS IMPROVED DRAMATICALLY, LOWERING DEATH RATES
In the early days, mortality for Covid was high because we didn’t know how to treat it. Death rates as a percentage of all cases has dropped dramatically.
https://www.cnbc.com/2020/06/23/better-coronavirus-care-younger-patients-means-fewer-will-die-gottlieb-says.html
New approaches to coronavirus care have helped lower mortality rate NJ hospital CEO says
https://www.cnbc.com/2020/07/21/nj-hospital-ceo-changes-in-coronavirus-care-have-lowered-mortality.html
Statins help reduce death rates
https://www.cell.com/cell-metabolism/fulltext/S1550-4131(20)30316-8
Covid patients suffer from oxygen deprivation much like altitude sickness and dexamethasone is the medicine for that. It lowers mortality.
https://www.forbes.com/sites/williamhaseltine/2020/06/16/dexamethasone-reduces-mortality-in-seriously-ill-covid-19-patients-and-so-do-other-treatments/
PUTTING COVID IN PERSPECTIVE
Globally
Currently, global deaths are 800,000 from Covid.
https://www.worldometers.info/coronavirus/
Globally, the World Health Organization (WHO) estimates that the flu kills 290,000 to 650,000 people per year.
https://www.health.com/condition/cold-flu-sinus/how-many-people-die-of-the-flu-every-year
So Covid is running a little over the upper end of world flu deaths annually.
Europe
180,000 people have died in all of Western Europe from Covid.
https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea
Here is a study of 2017/18 season.
It states that 152,000 people died during flu season from flu and unkown pathogens.
https://www.sciencedirect.com/science/article/pii/S1198743X19300588
The impact of the 2017/18 influenza epidemic on mortality was similar to that of the previous influenza A(H3N2) dominated seasons in 2014/15 and 2016/17. The European number of deaths attributable to influenza was estimated to be 152 thousand persons. We found a lower influenza-attributable mortality compared to excess mortality, which may indicated that other circulating pathogens might also have contributed to the all-cause excess mortality.
See the European flu monitoring site showing flu vs Covid. It isn’t twice as bad as previous bad flu seasons 2014/15 and 2017/18
https://www.euromomo.eu/graphs-and-maps
Italy had 35,00 Covid deaths.
https://www.worldometers.info/coronavirus/country/italy/
But Italy always has more deaths from influenza than other European countries.
It had excess deaths of 7,027 20,259 15,801 and 24,981 attributable to influenza epidemics in the 2013/14 2014/15 2015/16 and 2016/17 respectively
https://www.sciencedirect.com/science/article/pii/S1201971219303285
That means Covid was only 40% worse than their worst flu year in the last five years.
The UK had 46,000 deaths, from Covid
https://www.worldometers.info/coronavirus/country/uk/
For some perspective, there were 28,000 and 26,000 deaths from influenza in the UK in 2014 and 2017.
https://www.bbc.co.uk/news/health-34919149
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/839350/Surveillance_of_influenza_and_other_respiratory_viruses_in_the_UK_2018_to_2019-FINAL.pdf
So the end result is the virus is about 40% worse than a bad flu year.
France had 30,000 Covid deaths
https://www.worldometers.info/coronavirus/country/france/
That is only 60% worse than the 2014/15 flu season in France with 18,300 deaths.
https://fr.statista.com/infographie/11358/mortalite-de-la-grippe-en-france/
Spain had 28,000 Covid deaths
https://www.worldometers.info/coronavirus/country/spain/
But it has had about 15,000 deaths from flu in previous flu seasons, notably 2014/15
”Using population models, it has been estimated that in the last two seasons, the flu may have been responsible for up to 15,000 deaths attributable to this disease.”
https://www.elmundo.es/sociedad/2016/11/01/5818764746163f7e388b4573.html
The Instituto Nacional de Estadistica says 15,000 for last two seasons, so that is a bad year.
https://www.lne.es/espana/2020/06/15/gripe-causado-15000-muertes-espana/2647987.html
So Covid is basically twice as bad as a bad flu season in Spain.
The US has had 166,000 deaths from Covid.
https://www.worldometers.info/coronavirus/country/us/
The flu season in 2017-18 had a median estimate of 61,000 deaths, but upper bound of the estimate is 95,000 deaths.
https://www.cdc.gov/flu/about/burden/2017-2018.htm
The 2014-15 had 64,000 as top estimate for flu deaths.
https://www.cdc.gov/flu/about/burden/2014-2015.html
So Covid is roughly 60%-100% worse than the worst flu season we’ve had.
Another issue that is rarely mentioned is that Covid deaths and hospitalizations have been inflated. Here is the Irish Government’s analysis of Covid deaths. Many people had the virus but did not die of Covid.
Analysis of excess all-cause mortality in Ireland during the COVID-19 epidemic
https://t.co/g6Zuo1ICxg
Britain’s official death toll from the COVID-19 pandemic was lowered by over 5,000
https://www.nytimes.com/reuters/2020/08/12/world/europe/12reuters-health-coronavirus-britain-deaths.html
BEST SITES TO READ TO AVOID PANIC
They are worth bookmarking
https://swprs.org/a-swiss-doctor-on-covid-19/
See all the resources on the right tab. Also at the end of each post, they have a great Round Up of good articles and links.
Lockdown Sceptics is a great daily read.
https://lockdownsceptics.org
And a site that helps put things in perspective
http://inproportion2.talkigy.com/
And an American site.
https://rationalground.com/
MASKS?
Netherlands
https://news.yahoo.com/dutch-government-not-advise-public-180223717.html
Denmark
https://www.thelocal.dk/20200511/why-is-denmark-not-recommending-face-masks-to-the-public
Norway
https://www.fhi.no/globalassets/dokumenterfiler/rapporter/2020/should-individuals-in-the-community-without-respiratory-symptoms-wear-facemasks-to-reduce-the-spread-of-covid-19-report-2020.pdf