An Open Letter to Charlie Mitchell (Stuff)
In the year since New Zealand closed its border and adopted an ‘elimination strategy’ against SARS-Cov-2, only one reliable serology test has been conducted. During this period at least 47 serology studies have been conducted throughout the world. Serology tests were banned from import or sale in NZ.
The result of the authorised study of 9806 blood samples taken in December 2020, was pre-print published (not peer reviewed) on April 19: https://www.medrxiv.org/content/10.1101/2021.04.12.21255282v1
The headline result is that it found antibodies to SARS-CoV-2 in 0.1% of samples.
This is lower than we expected – especially when compared to the prevalence found in other nations of studies conducted earlier in the pandemic (as high as 50% in India). It is also much lower than the NZ prevalence of H1N1 (30% positive antibodies), which triggered health authorities to abandon elimination plans.
The title and commentary of the paper suggests this low level is explained by elimination of the virus. It is directly explained by the estimated 3-month half-life of antibodies (S and RBD, compared to month long half-life of N protein). Our reference paper on seropositivity is https://www.medrxiv.org/content/10.1101/2020.07.16.20155663v2.full.pdf. That means ‘fresh’ infections have been falling. This undoubtedly means that border closure has cut off supply of renewed infection but tells us very little about how much infection existed in NZ at the time of the border closure.
Even if you would like to believe the result shows the elimination strategy has throttled infection rates, you cannot ignore that it simultaneously proves that elimination is impossible. The 0.1% prevalence is double the number of identified positive tests. For every identified case, there is at least one other person with covid-19 who has not been identified. That means there has been at least 5000 cases in NZ (5,000,000*0.001).
Worse still, community infection is higher than thought. The study shows the ratio of previously detected locally acquired cases to known cases is 6:8. The number of locally acquired cases from the Ministry of Health is 2600 – 865 in MIQ = 1,735. This indicates that there were 2313 (1,735*8/6) extra locally acquired cases that were not detected.
If we wanted to ascertain true cumulative exposure to infection, then 0.1% is certainly an underestimate, compared to influenza antibodies. The study makes no mention of the possibility of infection that can be found in T-cell levels e.g. from Karolinska. Those studies suggest that if the true infection rate could be, conservatively, 1.5 times the antibody prevalence.
We note that the eight undetected cases claimed in media coverage were widely geographically distributed, so could not have been from a localised cluster. Covid-19 was evidently widespread across NZ, breaking the fiction of being contained by lockdowns and tracking into ‘clusters’.
A big implication of the study is that we now have a more definitive infection fatality ratio (IFR) for NZ of 0.5% (26/~5000). Only a month or two before this serology survey Rod Jackson and the NZ Herald refused to retract articles that told New Zealanders the IFR was at least double that (over 1%). We trust they will now delete those articles. Most other NZ experts have been more recently citing the CDC’s IFR of 0.65% – which is now clearly too high in NZ.
Our search for an accurate IFR now has a more certain starting point. We know that about one quarter of the NZ deaths were attributed to covid without evidence of a positive test. We also know that given the half-life of antibodies, the real infection level must be higher than 5000. A conservative level would be about 10,000 infections. So NZ’s IFR could be as low as 0.2% (20/10,000). This figure is concordant with median estimates from summaries of serology studies.
In summary, the study reveals a lower antibody level than we expected. It’s a surprise that indicates a likely waning of fresh transmission. But it reveals that we have had at least one undetected case for each detected case. This means:(a) the virus is not as deadly as first thought as these cases were not diagnosed since they didn’t come to clinical attention and(b) it is a fiction that New Zealand has detected each and every case of covid-19 and so can declare the virus ‘eliminated’.
Simon Thornley
18/04/2021
1014 words
In a recent interview with Radio New Zealand, a vaccine expert claimed that the risk of blood clot was 165,000 times higher after having covid-19, compared to the risk after having the AstraZeneca jab. This claim illuminates several misunderstandings of the nature of the SARS-CoV-2 virus, the true nature of the side effects that are worrying health officials overseas and the influence of misleading claims on social media.
Even though New Zealand is currently using a different vaccine, the emergence of blood clot reactions to some covid-19 vaccines has worried those who have been saying the vaccines are safe and effective.
In response they have tried to do something they refused to do with SARS-CoV-2; provide people with realistic data about the small risk posed.
To make the vaccine-related blood clots seem comparatively small, Dr Helen Petousis-Harris recently claimed that the risk of covid-19 blood clots was high.
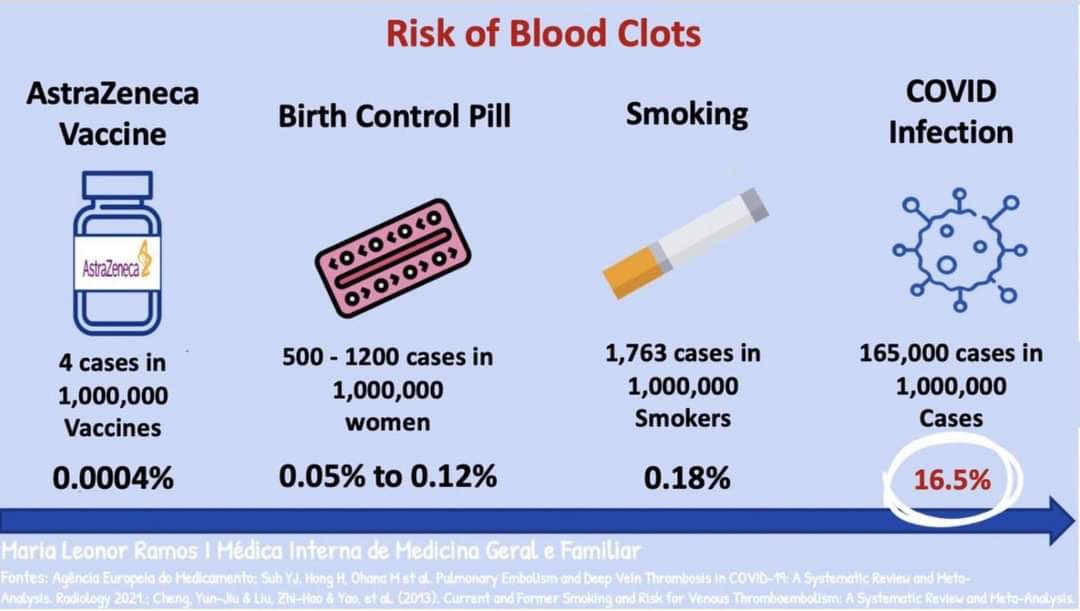
She said the risk of clot from the AstraZeneca vaccine is about 1/1,000,000 against risk of clotting from covid-19 which is 165,000/1,000,000.
The frequencies of 165,000/1,000,000 are hard to understand until we start wiping off a few confusing zeros and end up with 16.5/100 or 16.5%.
Dr Petousis-Harris claims that 1/6 people who have covid-19 infection have a clot; not just any clot, but the rare brain vein clot being experienced by covid-19 vaccine takers.
All Helen’s words are taken verbatim from numbers on an infographic image doing the rounds on social media.
The statistic of 1/6 people suffering rare clots after being infected with the covid-19 virus comes from a summary study of hospitalised patients which evaluated the risk of pulmonary embolus and deep vein thrombosis in patients hospitalised for covid-19. Over half the studies included in the summary were from patients in intensive care. Some studies screened all patients for clots. The average of all studies showed a weighted proportion of 16.5% for both deep vein (leg) and lung clots.
Despite widely held belief, over 95% of people who test positive for covid-19 do not need a hospital, so would not have appeared in the denominator of the 16.5% figure. A study from Iceland, one of the most tested nations on earth, showed that 5% of positive patients for covid-19 were hospitalised, and only 1% went to intensive care. This means that the 16.5% figure is a very skewed proportion of all patients with covid-19. Since only 1-5% of cases make it to intensive care or hospital, that 16.5% chance should be less than 1%.
We know also that many more people have caught the virus than the positive genetic (PCR) tests say, as shown by serological tests and other immune studies. T-cell tests show that even more have been exposed to the virus, compared to antibody studies. The incidence of blood clots following covid-19 infection is simply not known, but it must be at least an order of magnitude lower than presented by our vaccine expert. So now the claimed 16.5% chance of blood clots across the population is not even 1%; it is closer to 0.1%.
Now comes the worst part of this attempt to mislead people about the vaccine risk; we’re not even talking about the same type of blood clot.
The blood clots experienced by some vaccine takers is cerebral venous sinus thrombosis, a deadly and rare condition.
The blood clots that threaten about 0.1% of us who catch covid-19 is deep venous thrombosis, a comparatively common condition found across all manner of hospitalised patients. It is so common that in one autopsy case-series, 10% of deaths in hospital patients who had the post-mortem procedure were caused by venous thromboembolism.
The background rate of cerebral sinus thrombosis is estimated to be 1.32 per 100,000 person years.
In contrast, the background rate of deep venous thrombosis is estimated at 50/100,000 person years, about 38 times higher than for cerebral sinus clots. The risk of leg clots is very strongly age-related, with older people more affected.
A direct comparison of the rate of cerebral sinus thrombosis in covid-19 patients compared to those who have had covid-19 vaccines has been carried out. The rate of cerebral venous thrombosis was higher in the covid-19 group compared to the vaccinated, but by a factor of 6 rather than 165,000-fold higher, as claimed in the Radio NZ interview. The cerebral sinus thrombosis group after covid-19 was more likely to have heart disease than those who had had the virus without the clot. The covid-19 group only counted PCR positive individuals, which as mentioned, underestimates the spread of the virus. The rate of venous thrombosis in the vaccinated groups (both Pfizer and AstraZeneca) was about 4-5 per million people in the two weeks following the vaccine. The risk of the vaccine is clearly higher than baseline which is an annual statistic, even if it is lower than for people who have had covid-19.
The administrative bodies of several nations are rightly concerned about the incidence of a rare type of blood clot from the AstraZeneca vaccine. Concern is justified when one particular risk of taking the vaccine is higher or worse than the risk of not taking it.
The image carrying the numbers quoted by Dr Petousis-Harris has been shared over social media by New Zealand doctors. I am sure they were well-intentioned, but it is never justified to allay fears using false information. It is always wrong to misinform people, particularly over the risk to their health of a medical intervention.
I am severely disappointed that our national broadcaster has not questioned these statements. It concerns a vaccine New Zealand is not using. But what happens when it does? What happens if rare reactions and deaths are attributed to treatments used here? We must be able to count on our media, and taxpayer funded experts to look at data impartially.
The conversation they held with Dr Petousis-Harris revealed a hopelessly exaggerated view of the severity of covid-19 in the minds of our “experts”, doctors, and the governing elite.
I call on Dr Petousis-Harris and Radio NZ to check the numbers, issue a retraction and an apology.
Simon Thornley, Gerhard Sundborn.
12 April 2021
We are usually supporters of vaccines, and our children are all immunised.
Yet we have deep unease that the least tested vaccine in living memory, for a virus posing little risk to most people, has been purchased at great cost, and is being commended to New Zealanders as “safe and effective”.
When Covid Plan B opposed the elimination strategy a year ago, it was not because of doubts over vaccines. We said the strategy was too costly to pursue while waiting for a vaccine. We said that most solutions were likely to be unwarranted by the small danger posed by SARS-CoV-2.
The early development of vaccine-like products is a triumph of science.
Plan B had worried that vaccines would take years to pass the usual safety and effectiveness tests. We hadn’t counted on the panic being so strong that usual stages would be curtailed.
The speed, haste, and enthusiasm with which covid-19 vaccines have been thrust upon us has made us pause and examine the evidence.
New Zealand has purchased enough of the Pfizer mRNA vaccine for everyone in the country. Several other supply arrangements exist in case one falls through.
We do not know the cost of the vaccines, as it has been hidden from us. Sources overseas indicate the cost to governments of the Pfizer/BioNTech vaccine as US$19.50/dose – or NZ$27.63 at current exchange rates. So for 10 million doses, NZ may have paid NZ$276 million.
That doesn’t include the costs of distribution, cold-chain, quality control and administration of the jab.
Is this vaccine worth the cost? What is the evidence for the vaccine’s benefit and are there any potential downsides?
A primary factor in whether a vaccine is warranted for a particular disease in pre-covid times has rested on three principal factors. These are, among others:
The World Health Organization has released criteria which focus on clinical consequences, such as safety and efficacy, but also encompass other areas such as public health benefits such as the reduction of infection rate.
The document mentions the ‘preferred’ need for at least 70% vaccine efficacy, with consistent results in the elderly. 50% efficacy is considered minimal. The endpoint may be a combination of disease, severe disease, and or shedding or transmission. The document says 6 months of protection may be acceptable, but one year is preferable.
The WHO discussion of vaccine safety is vague. It says a ‘highly favourable benefit to risk profile’ is ideal, but the benefits outweighing the safety risks is ‘acceptable’.
A footnote mentions that the ‘potential for enhanced disease’ should be considered. Clearly, authors of the document are cognisant of the potential for antibody dependent enhancement, a phenomenon present for other viruses such as dengue, Zika, Ebola and other coronaviruses. This occurs when high antibody concentrations are initially effective against a pathogen, but waning immunity and lower concentrations paradoxically enhance the severity of infection.
The true cost of the epidemic is hard to pin down, and we’re yet to see a formal cost-benefit analysis of the effects of the vaccine, since the long-term effects of the product are unknown.
The main choice facing New Zealanders now is whether to be vaccinated with the Pfizer one, so we’ll focus on this. The main evidence relating to this vaccine is outlined in the New England Journal of Medicine. The trial randomly allocated ~40,000 participants, roughly half each into vaccinated and placebo groups and followed them for two months to see whether they developed covid-19 infection. The study excluded people under the age of 16, pregnant women and people with a history of either covid-19 or any immunocompromising condition. The primary outcome was defined by a positive PCR test, with at least one symptom of infection.
The headline results were 169/20,172 covid-19 events in the placebo group, compared to just 9/19,965 in the vaccine group, giving an efficacy of 94.6% after two months. The most reported side effects from the vaccine were transient, such as fatigue, headache, and muscle pain. The two-month trial did not address viral transmission nor long-term safety and effect.
The trial has come under scrutiny for unexplained incongruities. Further documentation has revealed that the rate of ‘suspected, but not confirmed’ covid-19 were similar between the two groups: with 1,594 cases in the vaccinated and 1,816 in the placebo.
There was also an imbalance in exclusions due to unexplained ‘protocol deviations’. In the vaccinated group 311 were excluded, compared to only 60 in the placebo. The chances of being excluded from the trial were therefore (311/21,720)/ (60/21,728) = 5.2 times higher in the vaccinated group, a ratio which is extremely unlikely to be due to chance (P < 0.001). This finding is buried in papers only made available to US regulators, rather than highlighted in the trial results. The selective exclusion of individuals in trials is an area commonly exploited by drug manufacturers to exaggerate claims. The best evidence conventionally comes from including all randomised subjects (‘intention-to-treat’), whether they deviate from the trial protocol or not. Requests for scrutiny of the trial data, to understand what factors lead to these exclusions, have been ignored.
Since the primary outcome of the trial is related to mild covid-19 events, we know little about whether the vaccine prevents deaths from the virus. Others have indicated that trials will not be sufficiently powered to detect differences in need for hospital treatment, let alone death from covid-19, since the number of subjects and resources required for such a trial would be prohibitive. We cannot assume that prevention of infection translates to fewer deaths. For influenza vaccinations, for example, even though they reduce infection, that has not translated into lower mortality after widespread uptake.
The vaccine has been studied in a healthy population who are largely unaffected by covid-19 hospitalisation or death, even with subjects drawn from supposedly ‘hard-hit’ regions, including the US, Brazil, South Africa, Germany, and Turkey. This trial evidence supports reductions in mild covid-19 infections only. We simply don’t know whether the vaccine will prevent what really matters: hospital and intensive care admissions and deaths.
The trial confirms that for people of working age, the risk of fatality from covid-19 is extremely low. So low in fact, that there will be too few deaths to run a trial without spending an extraordinary amount of money on a very large one. The conclusion by health authorities not to run a trial on vaccine effectiveness to prevent death means they themselves conclude that the fatality risk of the virus, and hence need for a vaccine, is overblown.
New Zealanders are being offered a covid-19 shot with the inaccurate assurance that it is “safe and effective”. From the evidence reviewed here, this message is disingenuous.
The long-term benefits and harms from covid-19 vaccines are unknown since they have only been recently used in humans. This is acknowledged in Medsafe’s 58 conditions for the emergency use. They require early alerts to company reports about the product’s safety and possible benefits. If the government’s own officials are sceptical and demand transparency, we should as well.
6 April 2021
By anonymous.
Like many gravitating to the Covid Plan B webpage, I am increasingly concerned about our government’s and indeed the global approach to the management of the Covid-19 pandemic. There are so many aspects of the present situation that seem so completely surreal.
From the philosophical perspective, I am deeply concerned about the adulteration of the scientific method. Am tired of hearing the media admonish us to trust the science and trust the experts. I constantly need to remind those around me that science is a tool, a method which if correctly applied will answer questions in a meaningful way bringing us progressively closer to an approximation of truth. It is primarily a process of observation and to make our observations meaningful these must be conducted in a carefully controlled manner.
By contrast, the force dominating our present world view is a deceitful yet carefully contrived facsimile of science. It uses all the vestiges, regalia and language of science without meeting the fundamental criteria. The policies and interventions which are being foisted upon us in the name of this pandemic are based not upon controlled observation, but rather upon narratives, rhetoric and data derived from some rather dubious uses of modelling. To make the distinction I will refer to this alternative paradigm of polemics and extrapolation as scientism. It is a sleight of hand, a wolf in sheep’s clothing, the proverbial cuckoo in the nest of the scientific method.
Examples of scientific fraud that have been perpetuated on our populous over the course of the present pandemic are sadly numerous. But I wish to focus here on the novel reversible gene therapy which is being deployed to our New Zealand population under the auspices of the disarming banner of the term “vaccine”. Vaccines are central to our medical approach to the prevention of severe human disease. However, the present technology has never been used for this application on prior occasions. It is disingenuous to include this technology within the trusted envelope of the term “vaccine” without evidence that it is both safe and effective for use in this capacity. The suggestion that an individual’s access to employment, ability to access services and ability to travel could depend upon their participation in this uncontrolled human experiment should be deeply alarming to anyone who places any value on human rights.
I have deep concerns about the speed at which these experimental “vaccines” are being presented as the only solution to the pandemic. No one has been able to answer the question as to how we can be confident that the recurring problem of antibody dependent enhancement which plagued our prior attempts to produce vaccines to other coronavirus variants in animal studies has been overcome. The main safety concern may not lie in the deployment of these “vaccines” but rather in the exuberance of the inflammatory response which follows the subsequent exposure of a patient to covid-19 or a future coronavirus variant.
Science aside, I am alarmed at the campaign of propaganda directed at the public through our mainstream media. The media’s phrasing of Covid-19 is hyperbole at best or worse – blatant fear mongering. By prefixing reports with phrase selection “the deadly virus” it is little wonder that many of our fellow New Zealanders are living in the state of fear that paralyses rational decision making. I am unaccustomed to living in an environment in which rational discussion has become verboten. Never have I seen anybody who dares to ask legitimate questions, shutdown so vehemently and labelled “controversial” or a “conspiracy theorist”.
It seems quite clear that we are only “allowed” to conform to the narrative being presented to us by our government and our trusted mainstream media. We once lived in a free society, with free speech and open dialogue, this no longer seems to be the case. Should we be concerned? I am.
The author: I do not wish to disclose my identity, at least for the time-being. I have undertaken a protracted tertiary education which includes degrees in science (cellular and molecular biology and biochemistry) medicine and dentistry and a doctoral degree with research in molecular biology. I am lucky to be a member of the fortunate educated.
Simon Thornley, Ananish Chaudhuri
1258 words.
António Egas Moniz was awarded the Nobel Prize in 1949 for frontal lobotomy, a supposed cure for mental illness. Ultimately, however, Moniz and the Nobel committee were wrong. The operation did irreparable harm to over fifty thousand patients and the results were far from the claimed ‘cure’.
Early in New Zealand’s Covid-19 story we were admonished with predictions of 80,000 covid-19 deaths by Professor Sean Hendy and his colleagues, even with stringent lockdowns in place. Recently, Professor John Gibson questioned the accuracy of these predictions as implausible because they would require our population to be almost 10-times larger, to square with the infection-fatality proportion reported by the WHO for countries like us. Yet Hendy doubled down on the predictions. Considering that New Zealand now has 26 official Covid-19 deaths, it seems at face value that Gibson is right. Hendy overshot the mark. By a lot.
What is remarkable now is the lack of insight into why these predictions were wrong. We have now learned so much more about Covid-19, we must update our ideas. The government’s own advice to its new Minister shows that Hendy’s exaggerated prediction will have enormous costs to New Zealand society. Crown debt is forecast to grow by 2.5 times to a level of NZ$200 billion in 2024, and the real value of output in 2020 is over five percent smaller than what had been forecast in 2019.
With so much at stake, it is essential that we take stock of what we have learned and why Hendy and his colleagues erred. After all, science is little more than the recalibration of our beliefs and predictions to match the stark reality of collected data. From what Hendy indicated in his response with revised predictions of 10,000 deaths he has learned little about the virus since the early forecasts. His response centred on explanations such as: vaccines arriving early, a modest change in the infection fatality rate (0.9% is the new value, compared to 1.0%), and the lack of capacity in intensive care.
What is most remarkable about these explanations is that none of them could possibly explain the discrepancy between Hendy’s original model and the observed deaths. Since the deaths are simply a proportion of the overall cases (infection fatality ratio), a 10% change can in no way explain the difference between models and reality, which differ by three orders of magnitude (3,076 times).
So, what have we learned about Covid-19 and why were Hendy’s models wrong? First, the models assumed the virus was totally new and that the entire New Zealand population was susceptible. Many studies now show that cross-reactivity and T cell responses to other coronaviruses protect us from Covid-19. Many of us will simply shake off the virus since our immune systems have already seen similar ones.
Hendy takes it as a given that Covid-19 is ten times more deadly than influenza, with no evidence cited. Calculating the ‘deadliness’ of a virus is a difficult issue, since it is dependent on accurately estimating cumulative numbers of infection – the denominator, as well as Covid-19 deaths – the numerator. Deaths are sensitive to definitions of what exactly constitutes a Covid-19 death, particularly in the frail elderly, who often have a range of other diseases.
To illustrate, Singapore has a strict definition of Covid-19 deaths, which requires a positive test and respiratory infection leading to death. The city state has registered only 30 deaths out of 60,019 cases (case fatality ratio: 0.05%). In contrast the UK, which has a comparatively loose definition, including all who died within a period of testing positive, has a case fatality ratio of 2.9%, 40 times higher than Singapore, from the same virus. The most comprehensive survey of infection fatality ratios, which account for positive serology, has yielded a corrected median of 0.23%, well under Hendy’s estimate. This figure does not account for T cell responses to the virus, and takes death recording at face value.
Evidence from wastewater in Barcelona and retrospective analysis of blood samples from a lung cancer screening study in Italy suggests that SARS-Cov-2 was circulating in Italy before its supposed discovery in Wuhan in December 2019. What do we learn from this? Since there was no excess death at that time, it cannot therefore be assumed that excess death that accompanied lockdowns is a direct consequence of the virus. Many of us have likely seen the virus and not known it, since it was circulating well before Wuhan, and health systems coped at that time.
It is remarkable also that Hendy’s doomsday predictions showed little appreciation of the age of deaths with Covid-19. Other authors predicted the magnitude of deaths in NZ from Covid-19 to those from World War 1, which averaged in the 20s of the soldiers who died. Spanish flu victims, similarly, had a median age of death in the twenties, but not those from Covid-19. The average age of deaths with Covid-19 are about the same as the life expectancy of that country. This means that the virus is certainly not as deadly as Hendy claims, since deaths from the virus will not lower the life expectancy of a population. Put another way, risk of death from the virus is no different to the background risks we face every day.
Hendy also fails to discuss the exaggeration in coding of Covid-19 deaths that has occurred during the pandemic. The fact that many deaths have been due to other illnesses and the usual process of recording death has been overturned. This panic induced exaggeration has also been a feature of many other historical epidemics of respiratory illnesses.
Another feature of the Covid-19 story is that much of the early high fatality was related to foregone opportunities for healthcare for other conditions. In the UK, emergency department visits halved during lockdown. To compound this, early mechanical ventilation in intensive care, which overloaded these units, inflated mortality from the virus. Statistical evidence now supports this policy as a cause of excess deaths in Covid-19 cases.
Hendy’s revised estimate that we must have saved at least 10,000 lives assumes lockdowns are effective. This is counter to the weight of statistical evidence on the subject. A between-country analysis showed no evidence that lockdowns save lives, either measured as a stringency index or from google mobility data.
We urgently need to return to the foundations of science which means a sober assessment of reality over failed forecasts. It seems Hendy is unlikely to champion such a cause, since his predictions have cost New Zealanders dearly. Wrong predictions are a routine part of science, but a stubborn adherence to them indicate a deviation from usual practise.
Our usual way of life, our ability to engage with the world, and much of our economy have been surrendered to erroneous predictions. Even with orders of magnitude differences from the reality of observed data, the author remains wedded to them.
The words of Nobel prize winner, Professor Richard Feynman are relevant:
“It doesn’t matter how beautiful your theory is, it doesn’t matter how smart you are. If it doesn’t agree with experiment, it’s wrong.”
Given what is at stake for New Zealand’s future, the last thing we now need is to cling to failed models. Rather, we must confront the frightening fact that much of what we initially thought we knew about Covid-19 was wrong. Dire predictions simply did not eventuate. The spectre of further lockdowns and strict border closures urgently need to be re-evaluated in this light. Feynman again:
“Reality must take precedence over public relations, for nature cannot be fooled.”
Simon Thornley
16/03/2021
Over a year now into New Zealand’s covid-19 saga, what can we learn from the experience of intensive care units? In the early days, protection of intensive care units and the scarcity of ventilators was a major factor shaping covid-19 policy.
New Zealand students were busy building ventilators, intensive care capacity was a major government concern, and became a key component of the elimination strategy.
The thought, early on, was that covid-19 was a completely new disease and that early mechanical ventilation was necessary in a patient’s treatment to give them a good chance to make it through. Since mechanical ventilation is a medical treatment, it must make things better, acting like a kind of super bellows, taking over when the patient ran out of steam, buying them time as their body beat back the virus.
The reality of intensive care experience has been somewhat different. It is well known that ventilators inflate the lung in an unnatural way, causing ventilator induced lung injury. They are far from a benign intervention and must only be applied sparingly.
Unfortunately, a certain level of jargon is necessary to dive deep into the ventilator story. A crucial measure of lung disease that is important in deciding to ventilate a sick or deteriorating patient is the ability of the lungs to soak up oxygen, known as the Pa02:FiO2 ratio. This is the ratio of oxygen pressure, measured from a patient’s artery relative to the percentage of oxygen being delivered, usually via a mask. This ratio indicates the ability of a patient’s lung to deliver essential oxygen to the body. Usually, values of 150 mmHg to 200 mmHg indicate the need for a ventilator. Early opinions from Wuhan, from Chinese anaesthetists, recommended early intubation, with patients having values as low as 300mmHg indicating need for a tube. In some hospitals, the milder form of breathing support, non-invasive ventilation, was not used due to the fear of spreading the virus to staff. In other areas, such as the US, financial incentives to ventilate were operating.
Early mechanical ventilation has been a spectacular failure, with the best evidence now showing that it did more harm than good. A recent study, published in January 2021, now has the wash-up from experience with 10,362 patients who have had covid-19 in the UK and been in through a critical care unit. These are covid-19 patients at the severe end. Almost 38% (3,933/10,362) of subjects died. The critical comparison was between those who were ventilated and those who were not. For those who were ventilated early, at low severity of lung disease (Pa02:FiO2 = 300mmHg), they had almost twice the rate of death, compared to those who weren’t, after accounting for all other factors. In fact, the most surprising finding was that for any level of lung impairment, those who were ventilated were more likely to die than those who were not. A conservative estimate of the importance of this finding, indicates that it accounted for about 15% or 1/7 of all the study deaths.
Naysayers may point out that the study was an observational one – not a trial – and that the results may be explained by doctors spotting unrecorded adverse factors that led them to put tubes down patients’ throats. An interview with North American intensive care doctors, however, contradicts this interpretation. Doctors spoke of asking patients to get off their mobile phones so they could put them on a ventilator. This was unusual practice, created by the fear of a new disease with an unpredictable course. Ultimately, it was learning to do less, rather than more which reduced mortality rates.
This created a sort of medical self-fulfilling prophecy of a deadly virus. The simplistic fixation on ventilators and the perceived need for them led to excessive use and premature deaths. Together with exaggeration of recording of covid-19 deaths, a vicious circle of fear took hold. The finding that Italy had ~10% of participants in a screening study of several regions of the country with antibodies for SARS-CoV-2 in September 2019, with no excess mortality at the time, strongly indicates that the healthcare and societal response, including lockdowns, were deadlier than the virus ever was.
“In ~ 98% of the comparisons using 87 different regions of the world we found no evidence that the number of deaths/million is reduced by staying at home. Regional differences in treatment methods and the natural course of the virus may also be major factors in this pandemic…”
The small sample size and the non-stationary nature of COVID-19 data are challenges for statistical models, but our analysis, with 25 epidemiological weeks, is relatively larger than previous publications which used only 7 weeks62. A short interval of observation between the introduction of an NPI and the observed effect on death rates yields no sound conclusion, and is a case where the follow-up period is not long enough to capture the outcome, as seen in previous publications44,45
given the importance of social isolation promoted by world authorities63, we expected a higher incidence of significant comparisons, even though it could be an ecological fallacy. The low number of significant associations between regions for mortality rate and the percentage of staying at home may be a case of exception fallacy, which is a generalization of individual characteristics applied at the group-level characteristics64.
Covid hysteria has highlighted the strange human tendency to want to believe the worst. No matter how bad something is, we are fascinated by the possibility it could be even worse.
Journalists are subject to the same psychological trait, but are also driven by their job to find material that escalates the fear.
An example is news coverage on whether SARS-CoV2 transmits from surfaces.
Media looked for people to confirm the possibility, then leaped onto research that confirmed it was possible.
Look at this shocking report on Reuters that focused on a CSIRO finding that Covid particles could live for up to 28 days. The report kicks off by saying the finding underlines the need for protective measures like hand-washing. The story includes video of HAZMAT suited research personnel running tests. The pairing of these signals effectively makes a conclusion from the research that live virus on surfaces is a real way of picking up a dangerous virus.
Information in the article which should provide context that lessens fear, such as mentioning it was a controlled environment, is present, but without any similar sort of conclusion for the average reader.
This is absolutely critical to the misleading nature of the story: the presentation of fear-inducing information (the fascinating news angle) is provided with scary comment and editorialising, but information that could lessen the fear is sparse and not explained.
Unfortunately, researchers live in the same world, influenced by the fear of authorities, funders and media. So there were motives to study surface transmission, and to highlight findings that suggested it was possible.
The CSIRO made almost no attempt to put the findings in context or lessen the hyperbole.
The result of these news reports to the public (and therefore to politicians and other authorities) that inflated and distorted the findings.
To be fair, some media did report properly. For example, it turns out that the CSIRO study was done in the dark! Light is a known anti-septic. The BBC noted this, but only after some experts were brave enough to point out these sort of context-relevant facts.
No media bothered reporting real world studies that found very short life spans for virus on surfaces.
Bizarrely, a Lancet piece as early as July highlighted the exaggeration of the risk. Emanuel Goldman concluded:
the chance of transmission through inanimate surfaces is very small, and only in instances where an infected person coughs or sneezes on the surface, and someone else touches that surface soon after the cough or sneeze (within 1–2 h). I do not disagree with erring on the side of caution, but this can go to extremes not justified by the data. Although periodically disinfecting surfaces and use of gloves are reasonable precautions especially in hospitals, I believe that fomites that have not been in contact with an infected carrier for many hours do not pose a measurable risk of transmission in non-hospital settings. A more balanced perspective is needed to curb excesses that become counterproductive.
By the November and December of 2020, the truth began to be properly reported. https://www.nytimes.com/…/world/asia/covid-cleaning.html.
It’s unclear what was going on that led to a media willingness to report this. Perhaps it might have been that there were sufficient other vectors for transmission that could be worried about. Certainly the mask issue was rampant at that time, with media backing up the official masking policies.
This coincided with another conclusive study in the Lancet. https://www.thelancet.com/…/PIIS2213-2600(20…/fulltext
Yet even in March 2021 the surface myth was persisting. Companies and organisations boasted of “deep cleaning” their premises in Auckland, NZ when the city locked down after covid cases were found and their movements tracked.
Even when being ‘critical’, media conformed to the surface-danger narrative. A New Zealand Herald story quoted a microbiologist warning that deep cleans were unlikely to get rid of the virus from the surface. Never mind that lots of research had already shown that the virus particles were unlikely to alive, or lead to infection, in the first place.
So it’s clear that media have not reported Covid information accurately or in context, fueling the Covid hysteria in 2020. They have been enabled in this by academics and researchers who either already distorted in their research, or found it difficult to convey the detail, or were drawn and mesmerized by the publicity into focusing on messages that made things look worse.
To top it off, most of us were almost gleeful to see the news, and convey to others: we thought it was bad, but it’s even worse than that!
***
{kind=link}